Vitamin B12
 Vitamin B12 (cobalamin), nature’s most chemically complex vitamin, also has been called its most beautiful, owing to the rich, dark red color of its crystals. But praise for the last B vitamin to be identified is hardly limited to its physical properties: B12’s vital role in the treatment of pernicious anemia has won it a dedicated following among physicians for decades. Vitamin B12 also has been shown to guard against stroke and heart disease, and contribute to relieving asthma, bursitis, depression, low blood pressure, multiple sclerosis, and even certain mental disorders. More recently, recognition of the essential role of one form of the compound—methylcobalamin—in supporting a variety of basic neurological functions has added to vitamin B12’s growing reputation as an indispensable supplement in the maintenance of a healthy mind and body.
Vitamin B12 (cobalamin), nature’s most chemically complex vitamin, also has been called its most beautiful, owing to the rich, dark red color of its crystals. But praise for the last B vitamin to be identified is hardly limited to its physical properties: B12’s vital role in the treatment of pernicious anemia has won it a dedicated following among physicians for decades. Vitamin B12 also has been shown to guard against stroke and heart disease, and contribute to relieving asthma, bursitis, depression, low blood pressure, multiple sclerosis, and even certain mental disorders. More recently, recognition of the essential role of one form of the compound—methylcobalamin—in supporting a variety of basic neurological functions has added to vitamin B12’s growing reputation as an indispensable supplement in the maintenance of a healthy mind and body.
Methylcobalamin helps moderate glutamate in the brain and support normal brain cell activity. Methylcobalamin also has been shown to encourage healthy cognitive, memory, and emotional function.1
 Picture 1:
Picture 1:
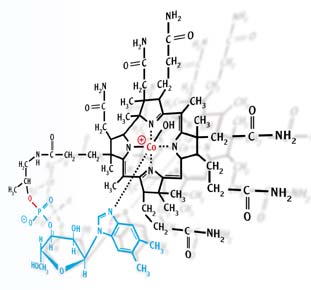
Photomicrograph of vitamin B12 cyanocobalamin), the most complex vitamin. It acts as a coenzyme in the synthesis of DNA and helps maintain proper cholesterol levels. Its deficiency leads to pernicious anemia and anorexia.
The Different Forms of B12
Vitamin B12 is one of the building blocks of life. Thought to play a primary role in the origin of DNA, cobalamin is involved in the synthesis of DNA, RNA, and molecules important for the maintenance of the genome.2 Cobalamin also is essential to the integrity and normal functioning of the nervous system.
Animal products are the principal food sources of B12, but paradoxically, plants and animals cannot produce the compound. Only bacteria are believed to manufacture the vitamin. Cobalamin actually is the collective term for four cobalt-containing compounds known as corrinoids. The term vitamin B12 typically is used to refer to cyanocobalamin, the main form of the vitamin typically used in nutritional supplements. Of the other three forms, methylcobalamin, one of the two coenzyme forms of cobalamin, is active in the central nervous system and is a vital cofactor in the conversion of homocysteine to methionine.
Central to Protein Synthesis
 Studies show methylcobalamin may play an important role in protein synthesis necessary for healthy cardiovascular function.3 Homocysteine, an amino acid formed when the body breaks down protein, is considered to be an independent risk factor for cardiovascular disease and stroke. Enzymes either turn homocysteine into the amino acid methionine, which can then be used to build more protein, or break it down in the urine for excretion. High levels of homocysteine may be toxic to the cells that line blood vessels, and also may increase clotting factors.
Studies show methylcobalamin may play an important role in protein synthesis necessary for healthy cardiovascular function.3 Homocysteine, an amino acid formed when the body breaks down protein, is considered to be an independent risk factor for cardiovascular disease and stroke. Enzymes either turn homocysteine into the amino acid methionine, which can then be used to build more protein, or break it down in the urine for excretion. High levels of homocysteine may be toxic to the cells that line blood vessels, and also may increase clotting factors.
Cobalamin deficiency leads to a reduced synthesis of methionine synthase, the key enzyme responsible for the conversion of homocysteine to methionine. The result is a high level of serum homocysteine and a decreased level of methionine.4
.jpg) Picture 2:
Picture 2:
Photomicrograph of macrocytes (overgrown red blood cells) reveals pernicious anemia in bone marrow cells. The disease is caused by a deficiency of vitamin B12 or a substance called an intrinsic factor (IF), produced by the lining cells of the stomach mucosa, which are necessary for the absorption of vitamin B12.
Benefits Beyond Anemia Treatment
 Vitamin B12 has long been associated with the treatment of anemia, but the neurological effects of B12 deficiency can occur even in the absence of anemia, particularly in those over the age of 60. Cobalamin deficiency principally affects the peripheral nerves, and in later stages may target the spinal cord. Impaired mental function is the usual result, often first manifesting as “slower thinking,” confusion, and memory lapses. Even a blood level of vitamin B12 that is moderately below the optimum can result in considerable damage to the brain and nervous system.5
Vitamin B12 has long been associated with the treatment of anemia, but the neurological effects of B12 deficiency can occur even in the absence of anemia, particularly in those over the age of 60. Cobalamin deficiency principally affects the peripheral nerves, and in later stages may target the spinal cord. Impaired mental function is the usual result, often first manifesting as “slower thinking,” confusion, and memory lapses. Even a blood level of vitamin B12 that is moderately below the optimum can result in considerable damage to the brain and nervous system.5
Moreover, it is now understood that a significant number of cognitive and emotional aptitudes depend on an optimal level of vitamin B12. In cognitive tests of elderly people, those who had the poorest scores had the lowest blood levels of vitamin B12. People diagnosed with depression have low plasma levels of cobalt, the mineral that forms the center of the vitamin B12 molecule.
B12 Absorption Declines with Age
 A primary determinant of the body’s ability to absorb B12 is a compound known as intrinsic factor, which is secreted by the cells lining the stomach. Intrinsic factor is crucial for absorption of cobalamin from the small intestine. The compound is produced in lesser amounts as the body ages, which accounts at least partially for the disproportionately larger incidence of vitamin B12 deficiency in elderly people—nearly one-third of people over the age of 60 cannot extract the vitamin B12 they need from the foods they eat.6 Stomach surgery or other conditions affecting the gastrointestinal tract also may affect production of intrinsic factor.
A primary determinant of the body’s ability to absorb B12 is a compound known as intrinsic factor, which is secreted by the cells lining the stomach. Intrinsic factor is crucial for absorption of cobalamin from the small intestine. The compound is produced in lesser amounts as the body ages, which accounts at least partially for the disproportionately larger incidence of vitamin B12 deficiency in elderly people—nearly one-third of people over the age of 60 cannot extract the vitamin B12 they need from the foods they eat.6 Stomach surgery or other conditions affecting the gastrointestinal tract also may affect production of intrinsic factor.
Another possible contributing factor is pernicious anemia, which severely reduces gastric secretion of intrinsic factor. In view of its association with a variety of antibodies, including at least two types of intrinsic factor antibodies, pernicious anemia is an autoimmune process. Intrinsic factor blocking antibody, which prevents the binding of vitamin B12 to the intrinsic factor molecule, is present in more than 50% of patients with pernicious anemia and only rarely is encountered in other conditions.7
Deciding Between Shots and Pills
 The time-honored method of addressing vitamin B12 deficiency is by injection. People suffering fatigue or the effects of alcohol overindulgence would simply go to the doctor for a vitamin B12 shot, and within a few hours might feel like new again. Injections are the preferred method for any condition that demands quick relief. But high dosages in pill form usually have the same effect.
The time-honored method of addressing vitamin B12 deficiency is by injection. People suffering fatigue or the effects of alcohol overindulgence would simply go to the doctor for a vitamin B12 shot, and within a few hours might feel like new again. Injections are the preferred method for any condition that demands quick relief. But high dosages in pill form usually have the same effect.
The problem with typical oral cobalamin supplementation is that the cobalamin may not be converted into adequate amounts of methylcobalamin required by the body to correct neural damage or decline.8
The easiest way around this problem is to bypass the liver entirely. Taking methylcobalamin sublingually (that is, dissolving it in tablet form under the tongue) allows the supplement to enter the bloodstream directly and has been shown to enhance absorption as much as fivefold.
 Optimal doses of vitamin B12 depend on the body’s needs, best determined by blood tests. The Schilling test, which uses a small dose of radioactive vitamin B12 that can be detected in the patient’s urine, is used to measure an individual’s ability to absorb the vitamin.
Optimal doses of vitamin B12 depend on the body’s needs, best determined by blood tests. The Schilling test, which uses a small dose of radioactive vitamin B12 that can be detected in the patient’s urine, is used to measure an individual’s ability to absorb the vitamin.
Vitamin B12 has been shown to be extremely safe and nontoxic, even in high doses. Everyday supplementation (300 to 1000 mcg) is a good starting point. Deficiency-related conditions require supplementing with at least 1 mg (1000 mcg) daily as part of a comprehensive nutrient program. According to recent data, supplementing with 2000 mcg per day addresses the symptoms of B12 deficiency, including elevated homocysteine and neurological problems.9,1
Material used with permission of Life Extension. All rights reserved.
1. Akaike A, Tamura Y, Sato Y, Yokota T. Protective effects of a vitamin B12 analog, methylcobalamin, against glutamate cytotoxicity in cultured cortical neurons. Eur J Pharmacol. 1993 Sep 7;241(1):1-6.
2. Verhoef P, Kok FJ, Kruyssen DA, et al. Plasma total homocysteine, B vitamins, and risk of coronary atherosclerosis. Arterioscler Thromb Vasc Biol. 1997 May;17(5):989-95.
3. Eikelboom JW, Lonn E, Genest J Jr, Hankey G, Yusuf S. Homocyst(e)ine and cardiovascular disease: a critical review of the epidemiologic evidence. Ann Intern Med. 1999 Sep 7;131(5):363-75.
4. Beyer K, Lao JI, Latorre P, et al. Methionine synthase polymorphism is a risk factor for Alzheimer’s disease. Neuroreport. 2003 Jul 18;14(10):1391-4.
5. Metz J. Cobalamin deficiency and the pathogenesis of nervous system disease. Annu Rev Nutr. 1992;12:59-79.
6. Harty RF, Leibach JR. Immune disorders of the gastrointestinal tract and liver. Med Clin North Am. 1985 Jul;69(4):675-704.
7. Irvine WJ. Immunoassay of gastric intrin- sic factor and the titration of antibody to intrinsic factor. Clin Exp Immunol. 1966 Jan;1(1):99-118.
8. Ide H, Fujiya S, Asanuma Y, Tsuji M, Sakai H, Agish Y. Clinical usefulness of intrathecal injection of methylcobalamin in patients with diabetic neuropathy. Clin Ther. 1987;9(2):183-92.
9. Schnyder G, Roffi M, Flammer Y, Pin R, Hess OM. Effect of homocysteine-lower- ing therapy with folic acid, vitamin B12, and vitamin B6 on clinical outcome after percutaneous coronary intervention: the Swiss Heart study: a randomized con- trolled trial. JAMA. 2002 Aug 28;288(8):973-9.
10. Shojania AM. How do you diagnose and manage vitamin B12 deficiency? Prairie Med J. 1994;64:141-2.
Related products
-
Methylcobalamin 1 mg
Price: 9,55 €The neurologically active form of vitamin B12 Essential for cell growth... -
BioActive Folate & Vitamin B12
Price: 12,53 €Promotes heart, brain, & GI tract health Helps promote healthy DNA... -

Methylcobalamin 5 mg
Price: 30,00 €The neurologically active form of vitamin B12 Vitamin B12 serum... -

Vitamin B12
Price: 12,07 €Essential vitamin B12 lozenges that dissolve in your mouth Vegetarians are...
Related posts
-
 Is Conventional Pomegranate Extract Enough?
An abundance of clinical data has established pomegranate as a broad-spectrum, multi-modal defense against the...
Is Conventional Pomegranate Extract Enough?
An abundance of clinical data has established pomegranate as a broad-spectrum, multi-modal defense against the... -
Feed Your Brain!
Millions of people around the world are adhering to low-fat, low-cholesterol diets in an effort to reduce the impact...
-
Lipoic Acid Reverses Mitochondrial Decay
It is estimated that 85% of the oxygen contained in every breath you take is consumed by the mitochondria within each...
-
Vitamin C and Dihydroquercetin
Every day, our bodies are under continual assault by damaging agents known as free radicals. Generally, both internal...
-
How Resveratrol Combats Leading Causes of Death
In 1997, the first scientific paper on resveratrol was published showing that this polyphenol could prevent cancer in...