Block The Deadly Effects Of Acid Reflux
 Those who complain about symptoms of acid reflux (heartburn) at least once a week are not alone. A startling 10 to 30% of Americans and Europeans may suffer symptoms of gastroesophageal reflux disease (GERD).1
Those who complain about symptoms of acid reflux (heartburn) at least once a week are not alone. A startling 10 to 30% of Americans and Europeans may suffer symptoms of gastroesophageal reflux disease (GERD).1
Although GERD is commonly treated with proton-pump inhibiting drugs such as Nexium® and Prilosec®,2 many patients using these medications do not achieve desired relief. Patients sometimes suffer rebound gastritis, develop a Helicobacter pylori infection, or encounter other adverse effects.1 These acid-blocking drugs are also linked to nutritional deficiencies, bone fractures, infections, and even withdrawal symptoms.3-8
While proton-pump inhibiting drugs do provide relief from distressing symptoms such as heartburn, regurgitation, difficulty swallowing, laryngitis, cough, and dental erosions1—acid reflux itself can have a lethal effect. Those with long-standing and severe acid reflux symptoms have 43 times the risk of developing esophageal cancer!9
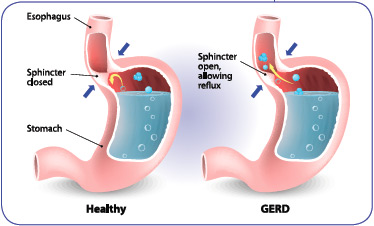
The main reason that proton-pump inhibitors don’t provide complete relief is that GERD is not caused by excessive stomach acid—GERD occurs when the sphincter valve between the stomach and esophagus fails to close completely. When this happens, undigested food and drink, bile, digestive enzymes, and stomach acids flow into the esophagus where they inflict considerable damage.
Once you understand that GERD involves more than just stomach acid, you’ll understand why it takes more than an acid-blocking drug to achieve optimal relief.
In this article, you’ll learn about a unique approach—known as raft-forming alginate10—that provides inclusive relief and protection from this chronic condition that affects so many aging individuals.11
Novel Approach Physically Blocks Acid Reflux
 A number of conditions increase the likelihood of acid reflux or GERD—a disorder in which the sphincter valve does not close sufficiently, thus allowing harsh stomach contents to wash back up into the delicate lining of the esophagus and throat.
A number of conditions increase the likelihood of acid reflux or GERD—a disorder in which the sphincter valve does not close sufficiently, thus allowing harsh stomach contents to wash back up into the delicate lining of the esophagus and throat.
Pregnancy can create temporary reflux, whereas obesity can result in chronic reflux.12
The number of people affected by acid reflux is expected to climb higher with the growing prevalence of reflux risk factors such as diabetes,13 asthma,13 being overweight,14 and greater use of ibuprofen, certain muscle relaxers, and blood pressure drugs.14
New findings reveal how acid reflux—as well as its inherent cancer and other health risks—can be blocked in a unique way.
Chewing tablets containing marine alginate and bicarbonate—known as raft-forming alginate10 —provides a temporary physical barrier that prevents the backwash of stomach contents, including burning acid, into the esophagus,11 thereby protecting delicate esophageal tissue.
Raft-Forming Alginate
 To provide relief to those suffering from acid reflux or GERD, doctors have been interested in strategies that not only cut the acid content of the stomach, but also block acid, enzyme, bile, and food reflux.15 Many patients with GERD exhibit food or acid reflux independently. A compound known as raft-forming alginate can decrease the number of both types of reflux events!
To provide relief to those suffering from acid reflux or GERD, doctors have been interested in strategies that not only cut the acid content of the stomach, but also block acid, enzyme, bile, and food reflux.15 Many patients with GERD exhibit food or acid reflux independently. A compound known as raft-forming alginate can decrease the number of both types of reflux events!
The alginate’s unique mechanism has been shown to work—often within a few seconds of dosing—to form a barrier that can be retained in the stomach for hours, providing longer-lasting relief than traditional antacids.11
When chewed, the alginate-based, raft-forming formulation expands in the stomach, where it mops up excess acid that is about to do damage to your esophagus and forms a pH-neutral barrier that reduces reflux episodes. Here’s how it works:
- One component of the mixture—alginic acid—is a dry powder derived from brown seaweed. Upon reaching the liquids and acid in the stomach, it forms a thick gel.11
- A second component of the mixture is sodium or potassium bicarbonate. On contact with gastric acids, it produces carbon dioxide bubbles that get trapped in the gel.11 The expanding bubbles cause the thick gel to form a foam that literally floats on top of the stomach contents like a raft.11
Scientists have shown that in people with acid reflux, the raft then glides up into the lower esophagus16 and creates a barrier that prevents acid and other stomach contents from pushing up into the esophagus.11
Meanwhile, the bicarbonate in the mixture reacts with the stomach acid and forms carbon dioxide—helping to directly neutralize stomach acidity. This provides an additional mechanism to further reduce the effects of heartburn.11
This entire raft-forming protective process occurs in less than a minute. Yet the raft can survive in the stomach for as long as four hours until it is finally broken up and passed out of the body.11 This explains raft-forming alginate’s remarkably rapid onset and long-duration relief when used immediately after a meal.11
In the next section, we’ll learn about compelling studies that have demonstrated that alginate is effective at reducing the intensity of symptoms and the frequency of reflux attacks.11,17
- Proton-pump inhibiting GERD drugs do not always provide sufficient improvement in acid reflux. They may cause rebound gastritis, H. pylori or C. difficile infection, and can increase the risk of nutritional deficiencies, bone fractures, and other complications.
- GERD causes heartburn, regurgitation, difficulty swallowing, laryngitis, cough, asthma, and dental erosions.
- Long-standing and severe GERD cases involve 43 times the risk of esophageal cancer.
- Proton-pump inhibitors don’t provide complete relief because GERD is not caused by excessive stomach acid, but by failure of the sphincter valve between the stomach and esophagus to properly close. This allows undigested food/drink, bile, digestive enzymes, and stomach acids to reflux into the esophagus where they inflict considerable damage.
- GERD is a strong risk factor for adenocarcinoma of the esophagus, which is on the rise compared to the squamous type of this cancer—and which is substantially more treatment-resistant than squamous carcinoma of the esophagus.
- A unique and effective approach offers both relief and optimum anticancer protection—raft-forming alginate physically blocks the backwash of stomach contents, including burning acid, into the esophagus.
Alginates Proven Effective In Human Studies
 Researchers set out to test on human patients the speed of relief provided by an alginate-based formula. They found that a single dose of a liquid form of alginate delivered a soothing effect in an average of just 65 to 66 seconds! Over 82% of patients described the effect as an “instant” cooling effect, and a full 100% of subjects experienced heartburn relief within just 3.3 minutes after the dose.18
Researchers set out to test on human patients the speed of relief provided by an alginate-based formula. They found that a single dose of a liquid form of alginate delivered a soothing effect in an average of just 65 to 66 seconds! Over 82% of patients described the effect as an “instant” cooling effect, and a full 100% of subjects experienced heartburn relief within just 3.3 minutes after the dose.18
In another study, addressing duration of relief, scientists employed sophisticated pressure- and acid-monitoring equipment to show that 20 mL of alginate kept the esophagus in the nonacidic range almost three times longer than placebo and slashed food reflux incidence in half.15
And in 2014, another comparison with a placebo was reported. This randomized, double-blind, clinical study on 110 GERD patients found that seven consecutive days of treatment with an alginate-containing formulation substantially decreased reflux and dyspeptic symptoms.19
Impressive results were also seen when alginates were experimentally compared to antacids and placebo.
Significant differences in objective scores—based on appearance and condition of the larynx—were seen between participants taking 10 mL of alginate suspension four times daily, after meals and at bedtime, relative to placebo subjects.20
Other studies demonstrated marked reduction in symptom severity scores and gastroesophageal reflux with alginates compared to the reflux medication Propulsid® (cisapride)21 and to the acid blocker Prilosec® (omeprazole).22
Since then, Propulsid® was removed from the United States market after it was shown to cause cardiac arrhythmias, with over 70 fatalities reported between 1993 and 1999.23,24 Side effects are also associated with Prilosec®.25-28 The good news is that a 2012 study published in BMC Gastroenterology showed that alginate treatment is equivalent to Prilosec®.29
In fact, studies regularly find that alginate treatment goes beyond superior efficacy—it delivers relief significantly faster than drugs.22,30
A huge benefit of alginate is that it erects a physical barrier that protects the esophagus—not only from stomach acid—but also from digestive enzymes, bile, and food/drink regurgitation. Proton-pump inhibiting drugs function only to stop acid production in the stomach.
Prevent GERD-Induced Cancer Of The Esophagus
 Many people think of the burning of GERD merely as pain and irritation—in other words, as a mere discomfort. But rates of esophageal cancer are rapidly increasing, and GERD is a major contributor.31,32
Many people think of the burning of GERD merely as pain and irritation—in other words, as a mere discomfort. But rates of esophageal cancer are rapidly increasing, and GERD is a major contributor.31,32
Esophageal cancers are most common in white men over 50, in smokers, in those who are obese, and especially in people with frequent symptoms of gastroesophageal reflux.33,34
Studies show that people with recurrent symptoms of reflux have a 7.7-fold risk of esophageal cancer, while those with long-standing, severe symptoms are at an incredible 43.5-fold risk of the disease!31
Worse, the prevalence of adenocarcinoma of the esophagus has been skyrocketing relative to squamous cell carcinoma of the esophagus35,36—which used to be the more common of the two.
The significance of this is 2-fold.
First, esophageal squamous cell carcinoma is largely attributed to cigarette smoking and excess alcohol ingestion,36-38 as well as infrequent consumption of raw fruits and vegetables39—while esophageal adenocarcinoma is known to occur more often in people with frequent symptoms of GERD.34
Second, and equally alarming, esophageal adenocarcinoma is substantially more resistant to treatment. In 2015, a Japanese medical team published a study indicating that the adenocarcinoma component of esophageal cancer is more stubbornly resistant to chemoradiotherapy than the squamous component of esophageal cancer.40
 When the sphincter valve at the bottom of your esophagus fails to close properly, stomach contents—including stomach acid and food—push up into the esophagus, causing heartburn and damaging the delicate esophageal lining. Drugs known as proton-pump inhibitors, such as Prilosec®, inhibit the release of stomach acid, providing some relief.50 However, the continual inhibition of acid release with drugs hinders digestion and absorption of key nutrients.51 This ultimately leads to alteration in gut pH balance and deficiencies in key nutrients, such as vitamin B12, iron, calcium, magnesium,52 folic acid,53 and zinc.54
When the sphincter valve at the bottom of your esophagus fails to close properly, stomach contents—including stomach acid and food—push up into the esophagus, causing heartburn and damaging the delicate esophageal lining. Drugs known as proton-pump inhibitors, such as Prilosec®, inhibit the release of stomach acid, providing some relief.50 However, the continual inhibition of acid release with drugs hinders digestion and absorption of key nutrients.51 This ultimately leads to alteration in gut pH balance and deficiencies in key nutrients, such as vitamin B12, iron, calcium, magnesium,52 folic acid,53 and zinc.54
The following are the most common adverse effects of proton-pump inhibitors:
- Blockage of release of a glycoprotein called “intrinsic factor,” making it impossible to absorb vitamin B12,
- Dietary iron is inhibited,55 contributing, over an extended period, to anemia,
- Calcium absorption is greatly reduced due to the reduced acid levels,52
- Active transport of magnesium in the intestine is inhibited,56 leading to deficiencies and potentially serious health consequences,
- Absorption of folic acid could be inhibited,53 disrupting production of new cells needed for body growth and repair,
- Impaired absorption of zinc,54 which is needed for a host of enzyme reactions in the body,57
- Increased risk of osteoporosis and bone fractures of any type, including wrist, spine, and hip,52
- Higher risk of infection—including pneumonia and C. difficile58,59—from decreased acid secretion and possibly from undigested food reaching the intestines and contributing to increased toxins and an imbalance of gut flora, and
- Withdrawal-induced rebound acid hypersecretion,60 forcing a return to drug usage.
Blocking Other GERD-Related Complications
 Aside from the much greater risk of a less treatable form of esophageal cancer, prolonged exposure of the esophagus to gastric reflux can cause dramatic alterations to its function. These serious complications of GERD can include peptic stricture41,42 or Barrett’s esophagus.43,44
Aside from the much greater risk of a less treatable form of esophageal cancer, prolonged exposure of the esophagus to gastric reflux can cause dramatic alterations to its function. These serious complications of GERD can include peptic stricture41,42 or Barrett’s esophagus.43,44
In people with long-term GERD, healing of ulcerations can lead to the deposit of fibrous scar tissue as well as a stricture—narrowing—of the esophagus known as peptic stricture.41 Segments of the esophagus with stricture are usually thickened, stiff, and may be shortened. The prevalence of peptic stricture among patients with GERD is about 10 to 25%.42 Treatment of severe peptic stricture involves the mechanical dilation of the narrowed region by a stent or balloon combined with acid suppression therapy.45
Barrett’s esophagus is a change in the cellular makeup of the mucous membrane of the esophagus. A normal esophagus is lined with a layer of flattened cells—squamous epithelial cells. In Barrett’s esophagus, these cells are replaced by a layer of thicker, taller cells—columnar epithelial cells, similar to those found on the inner surface of the stomach or intestines.46 The main cause of Barrett’s esophagus is thought to be an adaptation to chronic acid exposure from reflux esophagitis.43,44
Barrett’s esophagus can increase the risk of esophageal cancer.47 In fact, the risk of a patient with Barrett’s esophagus progressing to develop esophageal adenocarcinoma increases significantly with every year that Barrett’s persists.48,49
The optimum way to prevent these GERD-caused esophageal complications is to block the reflux of stomach contents into the esophagus in the first place—by relying on the physical barrier that alginate erects.
- Eating more slowly,
- Having more frequent, smaller meals,
- Avoiding fried foods,
- Limiting alcohol intake,
- Replacing sodas with health-promoting drink options,
- Lowering caffeine intake,
- Taking fewer prescriptions and over-the-counter medications,
- Watching for, and limiting, foods that aggravate symptoms,
- Quitting smoking,
- Not eating within two to three hours of bedtime,
- Maintaining a healthy weight level,
- Wearing looser-fitting clothes,
- Managing stress levels,
- Supplementing with digestive enzymes such as proteases and lipases (so that food is more quickly digested and leaves your stomach sooner),
- Taking 1-2 teaspoons of apple cider vinegar with water and raw honey to reduce symptoms,
- Taking quality probiotics to support healthy gut bacteria balance,
- Helping to protect your stomach and esophagus by taking d-limonene, an extract of the peels of citrus fruit, and
- Taking zinc-carnosine, cranberries, deglycyrrhizinated licorice, and picrorhiza for gastroprotective effects.
- Blood tests (complete blood count, comprehensive metabolic panel) to detect nutrient deficiencies,
- A high-quality calcium supplement, ideally combined with vitamins K and D3, and
- A high-quality multivitamin and mineral supplement with ample zinc dosage.
- Over-the-counter antacids can be effective against stomach-acid damage, but do not provide sufficient suppression of stomach acid, especially with prolonged use. Raft-forming alginate preparations provide effective physical barrier protection against reflux symptoms.
Summary
Proton-pump inhibiting drugs provide relief from distressing symptoms such as heartburn, regurgitation, difficulty swallowing, laryngitis, cough, and dental erosions. Yet gastroesophageal reflux (GERD) can have a lethal effect. Those with long-standing and severe acid reflux symptoms have 43 times the risk of developing esophageal cancer!
The reason that proton-pump inhibitors don’t provide complete relief is that GERD is not caused by excessive stomach acid. GERD occurs when the sphincter valve between the stomach and esophagus fails to properly close—allowing undigested food/drink, bile, digestive enzymes, and stomach acids to reflux into the esophagus and inflict considerable damage.
The fact that GERD involves more than just stomach acid explains why it takes more than an acid-blocking drug to achieve optimal relief.
GERD is a strong risk factor for adenocarcinoma of the esophagus, which is on the rise compared to the squamous type of this cancer—and which is substantially more treatment-resistant than squamous carcinoma of the esophagus.
Raft-forming alginate physically blocks the backwash of stomach contents, including burning acid, into the esophagus.
Material used with permission of Life Extension. All rights reserved.
- Patrick L. Gastroesophageal reflux disease (GERD): a review of conventional and alternative treatments. Altern Med Rev. 2011 Jun;16(2):116-33.
- Röhss K, Hasselgren G, Hedenström H. Effect of esomeprazole 40 mg vs omeprazole 40 mg on 24-hour intragastric pH in patients with symptoms of gastroesophageal reflux disease. Dig Dis Sci. 2002 May;47(5):954-8.
- Richards JB, Goltzman D. Proton pump inhibitors: balancing the benefits and potential fracture risks. CMAJ. 2008 Aug 12;179:306-7.
- Gulmez SE, Holm A, Frederiksen H, et al. Use of proton pump inhibitors and the risk of community-acquired pneumonia: A population-based case control study. Arc Intern Med. 2007 May 14;167(9):950-5.
- Bavishi C, Dupont HL. Systematic review: the use of proton pump inhibitors and increased susceptibility to enteric infection. Aliment Pharmacol Ther. 2011 Dec;34;(11-12):1269-81.
- Fossmark R, Johnsen G, Johanessen E, Waldum HL. Rebound acid hypersecretion after long-term inhibition of gastric acid secretion. Aliment Pharmacol Ther. 2005 Jan 15;21(2):149-54.
- Gray SL, LaCroix AZ, Larson J, et al. Proton pump inhibitors use, hip fracture, and change in bone mineral density in post-menopausal women: results from the Women’s Health Initiative. Arc Intern Med. 2010 May 2010;170(9):765-71.
- Eurich DT, Sadowski CA, Simpson SH, Marrie TJ, Majumdar SR. Recurrent community-acquired pneumonia in patients starting acid-suppressing drugs. Am J Med. 2010 Jan;123(1):47-53.
- Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999 Mar 18;340(11):825-31.
- Sweis R, Kaufman E, Anggiansah A, et al. Post-prandial reflux suppression by a raft-forming alginate (Gaviscon Advance) compared to a simple antacid documented by magnetic resonance imaging and pH-impedance monitoring: mechanistic assessment in healthy volunteers and randomised, controlled, double-blind study in reflux patients. Aliment Pharmacol Ther. 2013 Jun;37(11):1093-102.
- Mandel KG, Daggy BP, Brodie DA, Jacoby HI. Review article: alginate-raft formulations in the treatment of heartburn and acid reflux. Aliment Pharmacol Ther. 2000 Jun;14(6):669-90.
- Ranjitkar S, Kaidonis JA, Smales RJ. Gastroesophageal reflux disease and tooth erosion. Int J Dent. 2012;2012:479850.
- Available at: http://www.mayoclinic.org/diseases-conditions/gerd/basics/risk-factors/con-20025201. Accessed March 5, 2015.
- Available at: http://www.webmd.com/heartburn-gerd/guide/what-is-acid-reflux-disease#1. Accessed March 5, 2015.
- Washington N, Steele RJ, Jackson SJ, Washington C, Bush D. Patterns of food and acid reflux in patients with low-grade oesophagitis—the role of an anti-reflux agent. Aliment Pharmacol Ther. 1998 Jan;12(1):53-8.
- Quartarone G. Gastroesophageal reflux in pregnancy: a systematic review on the benefit of raft forming agents. Minerva Ginecol. 2013 Oct;65(5):541-9.
- Chatfield S. A comparison of the efficacy of the alginate preparation, Gaviscon Advance, with placebo in the treatment of gastro-oesophageal reflux disease. Curr Med Res Opin. 1999;15(3):152-9.
- Bordin DS, Masharova AA, Firsova LD, Kozhurina TS, Safonova OV. Evaluation of action, efficacy, and onset dynamics of a single dose of alginates in patients with heartburn and GERD. Eksp Klin Gastroenterol. 2009(4):77-85.
- Thomas E, Wade A, Crawford G, Jenner B, Levinson N, Wilkinson J. Randomised clinical trial: relief of upper gastrointestinal symptoms by an acid pocket-targeting alginate-antacid (Gaviscon Double Action)—a double-blind, placebo-controlled, pilot study in gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2014 Mar;39(6):595-602.
- McGlashan JA, Johnstone LM, Sykes J, Strugala V, Dettmar PW. The value of a liquid alginate suspension (Gaviscon Advance) in the management of laryngopharyngeal reflux. Eur Arch Otorhinolaryngol. 2009 Feb;266(2):243-51.
- Poynard T, Vernisse B, Agostini H. Randomized, multicentre comparison of sodium alginate and cisapride in the symptomatic treatment of uncomplicated gastrooesophageal reflux. Aliment Pharmacol Ther. 1998 Feb;12(2):159-65.
- Dettmar PW, Sykes J, Little SL, Bryan J. Rapid onset of effect of sodium alginate on gastro-oesophageal reflux compared with ranitidine and omeprazole, and relationship between symptoms and reflux episodes. Int J Clin Pract. 2006 Mar;60(3):275-83.
- Available at: http://www.rxlist.com/propulsid-drug.htm. Accessed March 9, 2015.
- Available at: http://dailymed.nlm.nih.gov/dailymed/archives/fdaDrugInfo.cfm?archiveid=13266. Accessed March 6, 2015.
- Reimer C, Bytzer P. Adverse events associated with long-term use of proton pump inhibitors. Ugeskr Laeger. 2012 Sep 24;174(39):2289-93.
- Odou P, Martin P, Membré S, et al. Omeprazole-induced leukopenia. A case report. J Clin Pharm Ther. 1999 Oct;24(5):317-21.
- Yu EW, Bauer SR, Bain PA, Bauer DC. Proton pump inhibitors and risk of fractures: a meta-analysis of 11 international studies. Am J Med. 2011 Jun;124(6):519-26.
- Howaizi M, Delafosse C. Omeprazole-induced intractable cough. Ann Pharmacother. 2003 Nov;37(11):1607-9.
- Pouchain D, Bigard MA, Liard F, Childs M, Decaudin A, McVey D. Gaviscon® vs. omeprazole in symptomatic treatment of moderate gastroesophageal reflux. a direc31comparative randomised trial. BMC Gastroenterol. 2012;12:18.
- Giannini EG, Zentilin P, Dulbecco P, et al. A comparison between sodium alginate and magaldrate anhydrous in the treatment of patients with gastroesophageal reflux symptoms. Dig Dis Sci. 2006 Nov;51(11):1904-9.
- Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999 Mar 18;340(11):825-31.
- El-Serag HB. Time trends of gastroesophageal reflux disease: a systematic review. Clin Gastroenterol Hepatol. 2007 Jan;5(1):17-26.
- Falk GW, Jacobson BC, Riddell RH, et al. Barrett’s esophagus: prevalence-incidence and etiology-origins. Ann N Y Acad Sci. 2011 Sep;1232:1-17.
- Thrift AP, Pandeya N, Whiteman DC. Current status and future perspectives on the etiology of esophageal adenocarcinoma. Front Oncol. 2012;2:11.
- Glenn TF. Esophageal cancer. Facts, figures, and screening. Gastroenterol Nurs. 2001 Nov-Dec;24(6):271-3.
- Available at: http://www.mdanderson.org/patient-and-cancer-information/cancer-information/cancer-types/esophageal-cancer/index.html. Accessed March 6, 2015.
- Lagergren J, Lagergren P. Recent developments in esophageal adenocarcinoma. CA Cancer J Clin. 2013 Jul;63(4):232-48.
- Ryan AM, Duong M, Healy L, et al. Obesity, metabolic syndrome and esophageal adenocarcinoma: epidemiology, etiology and new targets. Cancer Epidemiol. 2011 Aug;35(4):309-19.
- Bytzer P, Christensen PB, Damkier P, Vinding K, Seersholm N. Adenocarcinoma of the esophagus and Barrett’s esophagus: a population-based study. Am J Gastroenterol. 1999 Jan;94(1):86-91.
- Nozaki Y, Nishida T, Hori Y, et al. Chemoradiotherapy is effective for primary esophageal adenosquamous cell carcinoma but ineffective for the metastatic adenocarcinoma component. Nihon Shokakibyo Gakkai Zasshi. 2015;112(2):278-86.
- Rosemurgy AS, Donn N, Paul H, Luberice K, Ross SB. Gastroesophageal reflux disease. Surg Clin North Am. 2011;91(5):1015-29.
- Hoang CD, Koh PS, Maddaus MA. Short esophagus and esophageal stricture. Surg Clin North Am. 2005;85(3):433-51.
- Gerson L, Shetler K, Triadafilopoulos G. Prevalence of Barrett’s esophagus in asymptomatic individuals. Gastroenterology. 2002;123(2):461-7.
- Toruner M, Soykan I, Ensari A, Kuzu I, Yurdaydin C, Ozden A. Barrett’s esophagus: prevalence and its relationship with dyspeptic symptoms. J Gastroenterol Hepatol. 2004;19(5):535-40.
- Kamal A, Vaezi MF. Diagnosis and initial management of gastroesophageal complications. Best Pract Res Clin Gastroenterol. 2010;24(6):799-820.
- Chen H, Fang Y, Tevebaugh W, Orlando RC, Shaheen NJ, Chen X. Molecular mechanisms of Barrett’s esophagus. Dig Dis Sci. 2011;56(12):3405-20.
- Siersema PD. Pathogenesis, diagnosis and therapeutic possibilities of esophageal cancer. Curr Opin Gastroenterol. 2007;23(4):456-61.
- de Jonge PJF, van Blankenstein M, Looman CWN, Casparie MK, Meijer GA, Kuipers EJ. Risk of malignant progression in patients with Barrett’s oesophagus: a Dutch nationwide cohort study. Gut. 2010;59(8):1030-6.
- Wani S, Falk G, Hall M, et al. Patients with nondysplastic Barrett’s esophagus have low risks for developing dysplasia or esophageal adenocarcinoma. Clin Gastroenterol Hepatol. 2011;9(3):220-7.
- Gustavsson S, Mårdh S, Norberg L, Nyrén O, Wollert S. Omeprazole, cimetidine, and ranitidine: inhibition of acid production in isolated human parietal cells. Scand J Gastroenterol. 1985 Oct;20(8):917-21.
- Ito T, Jensen RT. Association of long-term proton pump inhibitor therapy with bone fractures and effects on absorption of calcium, vitamin B12, iron, and magnesium. Curr Gastroenterol Rep. 2010 Dec;12(6):448-57.
- Desmoulin SK, Hou Z, Gangjee A, Matherly LH. The human proton-coupled folate transporter: Biology and therapeutic applications to cancer. Cancer Biol Ther. 2012 Dec;13(14):1355-73.
- Ozutemiz AO, Aydin HH, Isler M, Celik HA, Batur Y. Effect of omeprazole on plasma zinc levels after oral zinc administration. Indian J Gastroenterol. 2002 Nov-Dec;21(6):216-8.
- Khatib MA, Rahim O, Kania R, Molloy P. Iron deficiency anemia: induced by long-term ingestion of omeprazole. Dig Dis Sci. 2002 Nov;47(11):2596-7.
- Cundy T, Dissanayake A. Severe hypomagnesaemia in long-term users of proton-pump inhibitors. Clin Endocrinol (Oxf). 2008 Aug;69(2):338-41.
- Maret W. Zinc biochemistry: from a single zinc enzyme to a key element of life. Adv Nutr. 2013 Jan 1;4(1):82-91.
- Wilhelm SM, Rjater RG, Kale-Pradhan PB. Perils and pitfalls of long-term effects of proton pump inhibitors. Expert Rev Clin Pharmacol. 2013 Jul;6(4):443-51.
- Biswal S. Proton pump inhibitors and risk for Clostridium difficile associated diarrhea. Biomed J. 2014 Jul-Aug;37(4):178-83.
- Lødrup AB, Reimer C, Bytzer P. Systematic review: symptoms of rebound acid hypersecretion following proton pump inhibitor treatment. Scand J Gastroenterol. 2013 May;48(5):515-22.
- Fossmark R, Johnsen G, Johanessen E, Waldum HL. Rebound acid hypersecretion after long-term inhibition of gastric acid secretion. Aliment Pharmacol Ther. 2005 Jan 15;21(2):149-54.
Related product
-
EsophaCool™
Price: 12,61 €On-the-go support for esophageal defense Supports a healthy inflammatory...
Related posts
-
 Turn Off Your Fat Switch: Deflating Your Spare Tire For a Longer, Leaner Life
If you’re like most Americans, you are struggling with at least a few extravpounds. And if you’re over 40, those...
Turn Off Your Fat Switch: Deflating Your Spare Tire For a Longer, Leaner Life
If you’re like most Americans, you are struggling with at least a few extravpounds. And if you’re over 40, those... -
Critical Need For a Multi-Modal Approach to Combat Obesity part 1
The scientific community now recognizes the role that obesity plays in the induction of age-related diseases and...
-
Critical Need For a Multi-Modal Approach to Combat Obesity part 2
Blocking the breakdown and absorption of carbohydrates are important points of intervention for losing weight. The...
-
Coffee. National Institutes Of Health Discovers Protective Effects Of Coffee
An exciting new study published in the New England Journal of Medicine suggests that coffee drinking may add years to...
-
Digestive Enzymes. Are You Obtaining the Proper Enzymes?
Even if you eat a healthy diet, you may not be absorbing vital fat-soluble nutrients and amino acids needed for...