Homocysteine Reduction
Summary and Quick Facts
 Elevated homocysteine levels in the bloodstream have been linked with a wide range of health problems.
Elevated homocysteine levels in the bloodstream have been linked with a wide range of health problems.- A high-protein diet, especially one that includes red meat and dairy products, can increase blood levels of homocysteine.
- If you have or are at risk for high homocysteine, the lifestyle strategies and homocysteine-lowering nutrients discussed in this protocol may help you achieve and maintain healthy homocysteine levels.
- Supplementation with B-vitamins, including folate, vitamin B6 and B12 have been shown in numerous studies to help lower homocysteine levels.
Homocysteine is an amino acid made from a common dietary amino acid, methionine, that inflicts damage to the inner arterial lining (endothelium). Elevated levels of homocysteine have been associated with many diseases, including:
- cardiovascular disease
- congestive heart failure
- stroke
- migraines
- age-related macular degeneration
- hearing loss
- brain atrophy
- Alzheimer disease
Fortunately, B vitamins like folate, vitamins B6 and B12, and other integrative interventions can reduce homocysteine and counteract this destructive process.
Causes of High Homocysteine Levels (Hyperhomocysteinemia)
 Many factors contribute to high homocysteine levels:
Many factors contribute to high homocysteine levels:
- Insufficient folate, vitamin B6, vitamin B12, betaine, vitamin B2, and magnesium
- Certain prescription drugs (including cholestyramine, colestipol, fenofibrate, levodopa, metformin, methotrexate, high-dose niacin, nitrous oxide, pemetrexed, phenytoin, sulfasalazine)
- High-methionine diet (including red meat and dairy products)
- Smoking
- High coffee consumption
- Alcohol consumption
- Advancing age
- Obesity
- Genetic variant that causes an impaired ability to metabolize active folate from folic acid
Note: Life Extension believes that the optimal range for homocysteine levels is <8 µmol/L, much lower than the currently accepted <15 µmol/L.
Dietary and Lifestyle Changes
Several dietary and lifestyle changes can help reduce chronic inflammation:
- Avoid methionine-rich foods like red meat and dairy products
- Exercise, as patients in a cardiac rehabilitation program showed a reduction in homocysteine from exercise alone
- Decrease or eliminate alcohol and smoking
Integrative Interventions
 B vitamins: Folate, along with vitamins B6 and B12, has been shown in numerous studies to help lower homocysteine levels. The active form of folate, L-methylfolate, can achieve plasma folate levels up to 700% higher than synthetic folic acid and therefore may be more effective at lowering homocysteine levels.
B vitamins: Folate, along with vitamins B6 and B12, has been shown in numerous studies to help lower homocysteine levels. The active form of folate, L-methylfolate, can achieve plasma folate levels up to 700% higher than synthetic folic acid and therefore may be more effective at lowering homocysteine levels.- Betaine (TMG) and choline: Higher intakes of TMG and choline (which is converted to TMG in the body) are related to lower circulating homocysteine concentrations.
- N-acetylcysteine (NAC): NAC may displace homocysteine from its protein carrier, which lowers homocysteine and promotes the formation of cysteine and glutathione, a powerful antioxidant.
- S-adenosylmethionine (SAMe): Supplementing with SAMe promotes the conversion of homocysteine to cysteine, which is then converted to glutathione and lowers homocysteine levels.
- Taurine: Research suggests taurine can block methionine absorption (which is converted to homocysteine in the body) and produce a significant decline in homocysteine levels in 4 weeks.
Introduction
 Homocysteine is an amino acid made in the body through metabolism of the essential amino acid methionine. In healthy circumstances, homocysteine is rapidly broken down, but genetic factors, nutritional inadequacies, certain medications, and some medical conditions can lead to excess homocysteine accumulation, which can damage blood vessels.1 High homocysteine levels have been correlated with a range of health problems, including atherosclerosis, stroke, neurological diseases, diabetes complications, osteoporosis, depression, erectile dysfunction, and pregnancy complications.2,3 Although the degree of causality attributable to homocysteine in these conditions is debated, maintaining a healthy homocysteine level is an important part of an overall healthy lifestyle. This is especially true in the context of cardiovascular and neurological health.3
Homocysteine is an amino acid made in the body through metabolism of the essential amino acid methionine. In healthy circumstances, homocysteine is rapidly broken down, but genetic factors, nutritional inadequacies, certain medications, and some medical conditions can lead to excess homocysteine accumulation, which can damage blood vessels.1 High homocysteine levels have been correlated with a range of health problems, including atherosclerosis, stroke, neurological diseases, diabetes complications, osteoporosis, depression, erectile dysfunction, and pregnancy complications.2,3 Although the degree of causality attributable to homocysteine in these conditions is debated, maintaining a healthy homocysteine level is an important part of an overall healthy lifestyle. This is especially true in the context of cardiovascular and neurological health.3
Adequate intake of the B vitamins folate (B9), cobalamin (B12), pyridoxine (B6), and riboflavin (B2) helps facilitate healthy breakdown of homocysteine.1 People with a genetic propensity for higher homocysteine levels may especially benefit from supplementing with B2, folate, B6, and B12.4 Omega-3 fatty acids may complement B vitamins in encouraging efficient metabolism of homocysteine.5 Betaine (also known as trimethylglycine, or TMG), magnesium, and the trace mineral lithium are also involved in maintaining homocysteine balance.6
In this protocol you will learn about methionine metabolism, factors that influence homocysteine regulation, and mechanisms by which excess homocysteine in the blood can cause harm. You will also learn the importance of monitoring homocysteine levels and effective methods for lowering high levels and protecting your long-term health.
Homocysteine Metabolism
 Although it is an amino acid, homocysteine is not derived from the diet. Instead, it is made inside cells from the essential dietary amino acid methionine.7 This process includes three steps:
Although it is an amino acid, homocysteine is not derived from the diet. Instead, it is made inside cells from the essential dietary amino acid methionine.7 This process includes three steps:
- Methionine to SAMe. Methionine is first converted into S-adenosylmethionine (SAMe) by adding a chemical group called an adenosyl group. SAMe is an important cellular methyl donor: it contains a methyl group that can be transferred to other molecules through methylation reactions. Methylation is critical in biosynthetic processes such as synthesis of DNA, RNA, and many amino acids, proteins, and phospholipids. Methylation is also a critical mechanism for modifying the structure of chromatin, which forms the backbone of deoxyribonucleic acid (DNA)—and which in turn determines how genetic material is expressed. This type of change that regulates gene expression, without changing the genetic code itself, is called epigenetics.
- SAMe to S-adenosylhomocysteine. When SAMe gives up its methyl group, the result is S-adenosylhomocysteine.
- S-adenosylhomocysteine to homocysteine. Through removal of the adenosyl group, S-adenosylhomocysteine is converted to homocysteine.
The Fate of Homocysteine
 About half of the homocysteine generated in cells is re-methylated, turning it back into methionine.8 In most of the body’s cells, this occurs via a folate-dependent pathway, in which a methylated form of folate (5-methyltetrahydofolate, or 5-MTHF) transfers its methyl group to homocysteine. The movement of a methyl group onto and off of folate involves vitamins B6, B2, and B12, as well as an important enzyme called methylenetetrahydrofolate reductase, or MTHFR.1,6,8
About half of the homocysteine generated in cells is re-methylated, turning it back into methionine.8 In most of the body’s cells, this occurs via a folate-dependent pathway, in which a methylated form of folate (5-methyltetrahydofolate, or 5-MTHF) transfers its methyl group to homocysteine. The movement of a methyl group onto and off of folate involves vitamins B6, B2, and B12, as well as an important enzyme called methylenetetrahydrofolate reductase, or MTHFR.1,6,8
Homocysteine can also be re-methylated via a folate-independent pathway, in which betaine (also known as trimethylglycine, or TMG) donates the methyl group to homocysteine. This occurs mainly in liver and kidney cells.1,6,8
Most of the homocysteine that is not re-methylated is converted to cystathionine via a chemical process called transsulfuration, which requires the amino acid serine, two important enzymes called cystathionine beta-synthase (CBS) and cystathionine gamma-lyase (CSE), and vitamin B6. Cystathionine can then be converted into the amino acid cysteine, or metabolized into energy.6 In addition to being used to make proteins, cysteine is also incorporated into the antioxidant glutathione.18,9
Causes of High Homocysteine Levels
Normally, about 5–10% of the homocysteine generated inside the cells is not metabolized and makes its way into the bloodstream and is subsequently cleared by the kidneys.9 However, when either re-methylation or transsulfuration are interrupted, more homocysteine moves out of cells and blood levels rise.8
Nutritional and Genetic Causes
Deficiencies of vitamins B2, B6, or, more commonly, B12 or folate interrupt re-methylation of homocysteine into methionine. Genetic alterations that result in less-efficient variants of the MTHFR enzyme also prevent sufficient homocysteine re-methylation. Importantly, when homocysteine re-methylation is impaired, SAMe levels fall, leading to a lack of methyl donors for other cell functions.8
Homocysteine transsulfuration can be interrupted when vitamin B6 intake is deficient or in cases of genetic mutations in the code for the CBS enzymes.8 The impairment of transsulfuration also leads to dysregulated hydrogen sulfide production.9
Other Causes
High homocysteine levels can result from any condition that restricts the availability of nutrients and energy for processing homocysteine. These include6,10-13:
|
|
In addition, several medications have been implicated in raising homocysteine levels. For example, antacids (H2 blockers such as ranitidine [Zantac] and cimetidine [Tagamet]), proton pump inhibitors (such as omeprazole [Prilosec] and esomeprazole [Nexium]), and metformin (Glucophage) can reduce vitamin B12 absorption and may increase homocysteine levels.14 The cholesterol-lowering drug fenofibrate (Antara, and others) and the blood pressure-lowering diuretic hydrochlorothiazide (Apo-Hydro, and others) have also been found to raise homocysteine levels.15
Consequences of High Homocysteine Levels
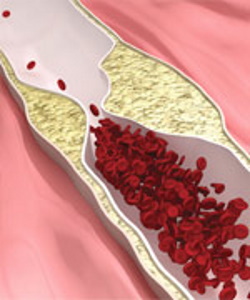 Although the exact mechanism of injury is still being investigated, it is clear that homocysteine has toxic effects on the cells that line the blood vessels. These cells (endothelial cells) are crucial for maintaining vascular tone and function and regulating inflammatory signaling in the blood vessel wall.1,8 Several damaging effects of excess homocysteine on endothelial cells have been demonstrated. These include1,8,9,16,17:
Although the exact mechanism of injury is still being investigated, it is clear that homocysteine has toxic effects on the cells that line the blood vessels. These cells (endothelial cells) are crucial for maintaining vascular tone and function and regulating inflammatory signaling in the blood vessel wall.1,8 Several damaging effects of excess homocysteine on endothelial cells have been demonstrated. These include1,8,9,16,17:
- Inhibiting antioxidant enzyme activity and raising levels of free radicals
- Disrupting normal production of nitric oxide and hydrogen sulfide, which help keep blood vessels relaxed
- Triggering mitochondrial dysfunction
- Increasing production of inflammatory cytokines
- Impairing methylation reactions
- Damaging the structure and function of proteins
Through these mechanisms, high homocysteine levels contribute to widespread vascular injury. This increases the risk of atherosclerosis, heart attack, and stroke, as well as cerebrovascular disease, cognitive decline, and dementia.16
Heart Disease
Research performed over the past two decades has established a clear link between high homocysteine levels and coronary artery disease, as well as acute heart failure, heart attack, and death for any reason in those with existing heart disease and in the general population.18-20 Some evidence suggests homocysteine may be a better indicator of cardiac risk than cholesterol.21 In fact, one meta-analysis calculated that every 5 µmol/L increase in homocysteine was associated with a 52% increased risk of death from coronary artery disease, 32% from cardiovascular disease, and 27% from any cause.19 High homocysteine is a predictor of onset of coronary artery disease, and may be an especially important biomarker of heart disease severity and prognosis in those affected at a younger age.22,23
Stroke
The toxic effects of homocysteine can contribute to formation of blood clots, and high homocysteine levels are associated with increased risk of stroke.12,24 In particular, having elevated homocysteine levels increases the risk of stroke four-fold in patients with atrial fibrillation, the most common cause of stroke in those over 80 years old.25 Furthermore, those who experience stroke are more likely to suffer from neurological deterioration within the first three days if their homocysteine level is high.26 Multiple controlled trials have indicated homocysteine-lowering therapy with vitamin B12 and/or folate can reduce stroke risk by at least 10%, with greater effects seen in those with higher homocysteine levels and lower folate status at baseline.12,27
Neurological Diseases
 By damaging the blood vessels that supply the brain, excess homocysteine in the blood can contribute to cerebrovascular cognitive decline, dementia, and Alzheimer disease. In addition, brain function depends on SAMe availability to run methylation reactions, and homocysteine accumulation is accompanied by SAMe depletion.26 Protein disruption and impaired epigenetic control of gene expression resulting from excess homocysteine further damages brain tissue.17
By damaging the blood vessels that supply the brain, excess homocysteine in the blood can contribute to cerebrovascular cognitive decline, dementia, and Alzheimer disease. In addition, brain function depends on SAMe availability to run methylation reactions, and homocysteine accumulation is accompanied by SAMe depletion.26 Protein disruption and impaired epigenetic control of gene expression resulting from excess homocysteine further damages brain tissue.17
High homocysteine levels have been shown to be correlated with an increased risk of Alzheimer disease and Parkinson disease.2 Individuals with elevated homocysteine levels are more likely to have markers of Alzheimer disease progression in brain tissue: neurofibrillary tangles, dysfunctional protein (amyloid-beta and phosphorylated tau) accumulation, and brain atrophy (shrinkage).28 According to one meta-analysis, every 5 µmol/L increase in homocysteine level is associated with a 15% increase in Alzheimer disease risk.29 In patients with Parkinson disease, elevated homocysteine is associated with worse cognitive function.30 Even modest elevation of homocysteine within the normal range (>11 µmol/L) has been associated with a substantial increase in risk of dementia in the elderly.28 Furthermore, lowering homocysteine levels using vitamins B12, B6, and folate has been found to markedly slow brain atrophy and cognitive decline.28
Other Conditions
 A number of other chronic conditions have been linked to high homocysteine levels. Importantly, the direction of causality between homocysteine and these conditions is not always clear, and more rigorous research is needed. Conditions associated with elevated homocysteine include:
A number of other chronic conditions have been linked to high homocysteine levels. Importantly, the direction of causality between homocysteine and these conditions is not always clear, and more rigorous research is needed. Conditions associated with elevated homocysteine include:
- Cancer. Cancer patients have higher levels of homocysteine compared with healthy people, and levels are higher in late stages than early stages of cancer. It is thought that genetic, epigenetic, and environmental factors each play a role, but the exact nature of this relationship is still being explored.31
- Diabetes complications. Due to the toxic effects of homocysteine on blood vessels, high homocysteine is linked to increased risk of cardiovascular and microvascular diabetes complications. This includes diabetic retinopathy (eye damage) and nephropathy (kidney damage).32,33
- Erectile dysfunction. A meta-analysis of findings from nine studies found men with erectile dysfunction were more likely to have high homocysteine levels than men without. This connection is most likely related to vascular damage induced by homocysteine.34
- Pregnancy complications. High homocysteine levels have been linked to increased risk of pre-eclampsia in pregnancy, a dangerous condition marked by high blood pressure and organ damage.35 High maternal levels of homocysteine are also associated with a range of congenital disorders, such as neural tube defects, cleft lip and palate, and Down syndrome.36
- Osteoporosis. Excess homocysteine has been shown to reduce both bone density and bone quality by damaging cells involved in bone turnover and interfering with the functionality of collagen.37
- Hearing and vision loss. High homocysteine levels have been linked to sensorineural hearing loss, a common cause of hearing loss in the elderly.38 Other findings suggest a possible link between elevated homocysteine levels and age-related macular degeneration, a frequent cause of vision loss.39
Homocysteine: Finding the Right Level
Homocysteine levels are usually measured using a blood test. Typically, the total amount of homocysteine, which includes free and protein-bound homocysteine, is reported.21 Total homocysteine levels of 5–14.5 µmol/L are generally considered normal; levels of 15–30 µmol/L are considered mildly elevated; 30–100 µmol/L are intermediately elevated; and levels exceeding 100 µmol/L are seriously elevated.2
Optimal Level
 The optimal level for homocysteine remains a topic of debate.40 Rather than there being a threshold above which disease occurs, the relationship between homocysteine levels and health may be more continuous.41-44 For this reason, Life Extension suggests most individuals strive to keep homocysteine levels below 12 µmol/L, with less than 8 µmol/L being considered ideal (although the latter may be difficult for some people to attain).
The optimal level for homocysteine remains a topic of debate.40 Rather than there being a threshold above which disease occurs, the relationship between homocysteine levels and health may be more continuous.41-44 For this reason, Life Extension suggests most individuals strive to keep homocysteine levels below 12 µmol/L, with less than 8 µmol/L being considered ideal (although the latter may be difficult for some people to attain).
Early homocysteine research attempting to identify the relationship between homocysteine and health noted that incremental increases in homocysteine levels were accompanied by a higher risk of cardiovascular disease and death.41,44 In one report from the Hordaland (Norway) Homocysteine Study, 4,766 participants aged 65–67 years had their homocysteine levels measured and were followed for 4.1 years. Compared to participants with homocysteine levels below 9.0 µmol/L, those with levels of 9.0–11.9 µmol/L had a 30% increased risk of cardiovascular death and 40% increased odds of non-cardiovascular death, and those with levels of 12.0–14.9 µmol/L had a 110% increased risk of cardiovascular and 90% increased risk of non-cardiovascular death. Furthermore, the risks were more than two-fold higher in those with levels of 15–19.9 µmol/L and more than three-fold higher in those with levels of 20 µmol/L and above.44 In people with coronary artery disease, similar rising trends in risk of hospitalization and death have been associated with incremental increases in homocysteine levels.42,43 A prospective case-control study of Japanese individuals aged 40 to 85 years found that stroke risk was significantly greater among individuals with homocysteine levels of 11 µmol/L or higher compared with those whose levels were less than 7 µmol/L.45
Homocysteine’s relationship with brain health may be similar, and individuals whose homocysteine levels are within the currently accepted normal range may still benefit from homocysteine-lowering therapy. In an eight-year study, participants with baseline homocysteine levels higher than 14.5 µmol/L had nearly twice the risk of Alzheimer disease compared to those with lower levels.46 Another study found elderly subjects with homocysteine levels of 10 µmol/L experienced marked cognitive deterioration when levels doubled to 20 µmol/L over 10 years.47
 A two-year randomized controlled trial assessed the rate of brain atrophy in 168 individuals over age 70 who had mild cognitive impairment and were given a placebo or B-vitamin supplementation (0.8 mg folic acid, 500 mcg B12, and 20 mg B6) daily. The researchers found that the rate of brain atrophy was considerably slower in the B-vitamin group compared with the control group. Importantly, the treatment response was related to baseline homocysteine levels such that individuals with levels above 13 μmol/L exhibited greater reductions in the rate of brain atrophy with B-vitamin supplementation than those with lower homocysteine levels. The researchers noted that homocysteine-lowering therapy with B vitamins was beneficial in those with baseline homocysteine levels of 9.5 µmol/L or higher.48 Furthermore, research from 1997 found that, in healthy men, folic acid supplementation reduced homocysteine levels in all tertiles except the lowest tertile, in which average baseline levels of homocysteine were 7.07 µmol/L.49 Cumulatively, these findings suggest supplementation with homocysteine-lowering B vitamins may confer benefits even among individuals whose homocysteine does not exceed normal lab reference ranges.
A two-year randomized controlled trial assessed the rate of brain atrophy in 168 individuals over age 70 who had mild cognitive impairment and were given a placebo or B-vitamin supplementation (0.8 mg folic acid, 500 mcg B12, and 20 mg B6) daily. The researchers found that the rate of brain atrophy was considerably slower in the B-vitamin group compared with the control group. Importantly, the treatment response was related to baseline homocysteine levels such that individuals with levels above 13 μmol/L exhibited greater reductions in the rate of brain atrophy with B-vitamin supplementation than those with lower homocysteine levels. The researchers noted that homocysteine-lowering therapy with B vitamins was beneficial in those with baseline homocysteine levels of 9.5 µmol/L or higher.48 Furthermore, research from 1997 found that, in healthy men, folic acid supplementation reduced homocysteine levels in all tertiles except the lowest tertile, in which average baseline levels of homocysteine were 7.07 µmol/L.49 Cumulatively, these findings suggest supplementation with homocysteine-lowering B vitamins may confer benefits even among individuals whose homocysteine does not exceed normal lab reference ranges.
Treatment
B vitamins are the main therapeutic agents used to treat high homocysteine levels. Many studies confirm their ability, alone and in combinations, to lower high homocysteine levels, and some trials show clinical benefits in the form of reduced risk of stroke and dementia. In general, the combined use of vitamin B12 and folate is more effective than either alone. Benefits of including vitamins B6 and B2 in homocysteine-lowering treatment have also been reported.12,24
Vitamin B9: Folate
 Folate, sometimes referred to as vitamin B9, is found in many plant foods, but is often lost or degraded through cooking and processing.56 In addition, intake is frequently low, especially in older individuals.57 Folate deficiency is associated with cognitive decline, depression, and neuropathy.58,59 There is also evidence linking poor folate status with epigenetic disturbances associated with Alzheimer disease.60
Folate, sometimes referred to as vitamin B9, is found in many plant foods, but is often lost or degraded through cooking and processing.56 In addition, intake is frequently low, especially in older individuals.57 Folate deficiency is associated with cognitive decline, depression, and neuropathy.58,59 There is also evidence linking poor folate status with epigenetic disturbances associated with Alzheimer disease.60
Adequate folate status is needed to re-methylate homocysteine into methionine. Supplementation with folic acid in amounts of 0.5–5 mg per day has been found to reduce homocysteine levels by around 25%. Because of the close relationship between folate deficiency and neural tube birth defects, mandatory fortification of grain products was introduced in the United States in 1998. Since that time, homocysteine levels in middle-aged adults has fallen by approximately 7%.61
Folic acid supplementation has been found in multiple studies to improve cognitive function, particularly in people with high homocysteine levels.62 Meta-analyses of clinical trials have reported that lowering homocysteine levels with folic acid therapy reduces risk of stroke by an average of 10% and all cardiovascular events by 4%. These benefits are correlated with degree of homocysteine reduction and are more evident in those with lower baseline folate levels.61,63 A meta-analysis of 49 randomized controlled trials found taking folic acid plus blood pressure-lowering medication was more effective than blood pressure-lowering medication alone in lowering blood pressure and reducing risk of cardiovascular events and stroke in subjects with high blood pressure. The benefits were greatest in those who took folic acid for more than 12 weeks and those whose homocysteine levels dropped by more than 25%. 64 Folic acid may be less helpful in those with metabolic disease since meta-analyses of trials in participants with type 2 diabetes and other metabolic disorders found that folic acid improved insulin sensitivity, but had no impact on blood pressure, fasting glucose levels, blood glucose control, or lipid levels.65,66
The Importance of Choosing L-methylfolate over Folic Acid
 Supplements are usually made with the shelf-stable synthetic version of folate, folic acid, which in most people is readily converted to the form used in the body, 5-methyltetrahydrofolate (5-MTHF). However, a substantial percentage of the population has one or more genetic variations that interfere with the efficient transformation of folic acid to 5-MTHF.67
Supplements are usually made with the shelf-stable synthetic version of folate, folic acid, which in most people is readily converted to the form used in the body, 5-methyltetrahydrofolate (5-MTHF). However, a substantial percentage of the population has one or more genetic variations that interfere with the efficient transformation of folic acid to 5-MTHF.67
L-methylfolate is a form of folate available in some supplements that is already in the 5-MTHF form. This means that the L-methylfolate form does not require the MTHFR enzyme to create functional folate to be used in homocysteine metabolism.68 People with these inefficient MTHFR genetics benefit more from L-methylfolate than from synthetic folic acid supplements.69 Even people with normal MTHFR genetic status have been shown to respond better to the L-methylfolate form compared with conventional synthetic folic acid.70-74
Importantly, it has been demonstrated that high-dose synthetic folic acid can prevent proper folate metabolism in both normal individuals and people with 5-MTHFR genetic variants.75,76 Fortunately, supplementation with L-methylfolate avoids this problem altogether.
Vitamin B12: Cobalamin
Vitamin B12, or cobalamin, is found in various forms in food and supplements, all of which are broken down to release free cobalamin. Cobalamin is transported into cells, where it can be converted into methylcobalamin, the active form needed for homocysteine metabolism.77 B12, in the form of cyanocobalamin, hydroxocobalamin, or methylcobalamin, is often administered as intramuscular injections due to low absorption in the digestive tract; however, there is some evidence showing oral doses of 1,000–2,000 mcg per day may be effective for normalizing low blood levels of vitamin B12.78,79
The most common test for B12 status is total serum B12; however, because only ~6–20% of B12 in the blood is metabolically active, even people with total B12 levels in the normal range may have inadequate active B12.25,80,81 While the normal range is generally 160–950 picograms/mL (or 118–701 picomoles/L),82 a B12 level of at least 540 picograms/mL (400 picomoles/L) is needed to keep homocysteine levels from rising. The combination of a B12 level in the lower half of the normal range plus an elevated homocysteine level is indicative of metabolic B12 deficiency.25
 The close relationship between vitamin B12 and folate makes it difficult to distinguish their independent deficiencies and therapeutic effects. Vitamin B12 deficiency causes a functional folate deficiency by “trapping” folate as 5-methyltetrafolate, preventing its use for other functions. On the other hand, supplementing with folate can “mask” a B12 deficiency by normalizing changes to red blood cells that are often an early sign of B12 deficiency.83
The close relationship between vitamin B12 and folate makes it difficult to distinguish their independent deficiencies and therapeutic effects. Vitamin B12 deficiency causes a functional folate deficiency by “trapping” folate as 5-methyltetrafolate, preventing its use for other functions. On the other hand, supplementing with folate can “mask” a B12 deficiency by normalizing changes to red blood cells that are often an early sign of B12 deficiency.83
Clinical evidence shows supplementing with B12 at doses of up to 1,000 mcg per day can safely reduce homocysteine levels in B12-deficient subjects, and the effect is enhanced as the dose increases.84,85 Low serum B12 levels have been linked to high blood pressure and neurological disorders, whereas maintaining higher B12 levels appears to protect against brain tissue atrophy (shrinkage) and may help prevent depression, particularly in the elderly.86,87 Including B12 in homocysteine-lowering therapy increases treatment efficacy and reduces stroke risk.12,25 It is important to note that some evidence indicates repeated high doses of cyanocobalamin may be harmful in those with kidney disease; therefore, methylcobalamin and hydroxocobalamin are preferable forms for vitamin B12 therapy.25
Vitamin B6: Pyridoxine
 Vitamin B6 (pyridoxine) is a cofactor in more than 140 reactions in cells, including both the re-methylation and transsulfuration of homocysteine. Although vitamin B6 is widely available in foods, intake has been shown to be low in as many as 31% of non-institutionalized older adults in Western countries.57 Low B6 status can cause homocysteine accumulation and reduce SAMe availability for methylation reactions, leading to reduced neurotransmitter synthesis and associated mood and neurological problems.88 Few studies have examined the role of vitamin B6 on homocysteine-related disorders independently of folate and B12, but a meta-analysis determined higher intake of B6 is correlated with lower risk of coronary heart disease.89
Vitamin B6 (pyridoxine) is a cofactor in more than 140 reactions in cells, including both the re-methylation and transsulfuration of homocysteine. Although vitamin B6 is widely available in foods, intake has been shown to be low in as many as 31% of non-institutionalized older adults in Western countries.57 Low B6 status can cause homocysteine accumulation and reduce SAMe availability for methylation reactions, leading to reduced neurotransmitter synthesis and associated mood and neurological problems.88 Few studies have examined the role of vitamin B6 on homocysteine-related disorders independently of folate and B12, but a meta-analysis determined higher intake of B6 is correlated with lower risk of coronary heart disease.89
Vitamin B6 is only active in its phosphorylated form, pyridoxal 5-phosphate (P5P), and supplementing with this form may be more effective for improving B6 status in some cases.90 Most supplements contain pyridoxine, which is readily transported across cell membranes and phosphorylated.77 Taking excessively high doses of vitamin B6 for prolonged periods can cause nerve symptoms that resemble deficiency, but some evidence suggests only the pyridoxine form is linked to this toxic effect.91
Vitamin B2: Riboflavin
Vitamin B2 (riboflavin) intake and blood levels are frequently low in older people.57,92 B2 is a cofactor for numerous cellular enzymes, including two enzymes involved in re-methylation of homocysteine: methylenetetrahydrofolate reductase (MTHFR, which helps activate folate to act as a methyl donor) and methionine synthase reductase (MTRR, which works with vitamin B12 to promote homocysteine re-methylation).1 Homocysteine levels rise with declining riboflavin intake and blood levels.85 Riboflavin supplementation may have a positive impact on homocysteine metabolism, particularly in individuals with the MTHFR genetic variant that affects the folate cycle.4,53 In addition, treating high homocysteine levels with folate alone can deplete vitamin B2 regardless of MTHFR genotype, lowering the potential efficacy of folate therapy.93
B Vitamin Combinations
Vitamins B2, B6, B12, and folate are inextricably linked through their interdependent roles in homocysteine metabolism and the fueling of methylation pathways. Their close functional relationship is illustrated by the fact that their deficiency syndromes share many symptoms. Regardless of their interrelatedness, most research has examined the homocysteine-lowering abilities of B vitamins independently, with the greatest emphasis on folic acid, followed by B12 and B6, respectively, with very little attention on B2. The potential benefits of supplementing with a full complement of B vitamins has been largely unexplored.85
In one randomized controlled trial, supplementing with 500 mcg B12, 800 mcg folic acid, and 20 mg B6 daily for two years reduced atrophy of gray matter (brain tissue most vulnerable to Alzheimer’s pathology) seven-fold in patients with mild cognitive impairment and high baseline homocysteine levels.94
One controlled trial demonstrated the superiority of a combination B vitamin supplement over folic acid alone. In the trial, 104 participants with high blood pressure and high homocysteine levels received either 5 mg folic acid per day or a daily supplement providing 400 mcg folate (as 5-methyltetrahydrofolate), 5 mcg B12, 3 mg B6, and 2.4 mg B2, as well as 12.5 mg zinc and 250 mg betaine. Average homocysteine levels fell from 22.6 to 14.3 µmol/L in the folic acid group and from 21.5 to 10.0 µmol/L in the combination group. Furthermore, more than 55% of those taking the combination supplement attained homocysteine levels of <10 µmol/L, which the study authors considered ideal.95
Nutrients
In addition to B vitamin therapy described in the “Treatment” section, several nutritional supplements have been shown to be helpful in people with high homocysteine levels.
Choline and Betaine
 Choline is a nutrient found in many foods such as egg yolks, dairy products, meat, peanuts, cruciferous vegetables, nuts and seeds, whole grains, and soybeans. It is an important structural component of cell membranes, a precursor for the neurotransmitter acetylcholine, and an integral part of brain tissue. Choline can also be used to make betaine, or trimethylglycine, which acts as a methyl donor.113 Betaine is a cofactor in the re-methylation of homocysteine into methionine, particularly in the absence of adequate folate.113 In addition to being made in the body, betaine occurs in foods like seafood, wheat germ and bran, beets, and spinach.114
Choline is a nutrient found in many foods such as egg yolks, dairy products, meat, peanuts, cruciferous vegetables, nuts and seeds, whole grains, and soybeans. It is an important structural component of cell membranes, a precursor for the neurotransmitter acetylcholine, and an integral part of brain tissue. Choline can also be used to make betaine, or trimethylglycine, which acts as a methyl donor.113 Betaine is a cofactor in the re-methylation of homocysteine into methionine, particularly in the absence of adequate folate.113 In addition to being made in the body, betaine occurs in foods like seafood, wheat germ and bran, beets, and spinach.114
Inadequate intake of choline and betaine can result in reduced production of SAMe and increased accumulation of homocysteine. This imbalance impairs methylation processes in cells, leading to breakdown in cellular function and epigenetic changes to DNA.115
Betaine plays a critical role in regulating homocysteine levels, especially in low folate, low B12, and high methionine conditions.116,117 Despite its presence in many and various foods, the NHANES found less than 11% of Americans achieve the recommended intake for choline, which is 550 mg per day for men and 425 mg per day for women.118
Betaine supplementation, at doses of 1,000–6,000 mg per day, has been shown to lower blood homocysteine levels and moderate the increase in homocysteine that follows ingestion of methionine.119-121 In a placebo-controlled trial in 23 athletes, those given 2,500 mg betaine per day during a six-week exercise training program had a lower exercise-induced rise in urinary homocysteine thiolactone, a form of homocysteine known to have toxic effects on blood vessels and interfere with normal protein production and function.122,123 It is important to note, however, the effect of high intake of choline and betaine on cardiovascular disease risk and mortality is unclear.124,125
Omega-3 Fatty Acids
 Omega-3 fatty acids appear to work synergistically with B vitamins to promote healthy homocysteine metabolism and reduce risk of conditions associated with high homocysteine levels, including cardiovascular and neurological diseases.5 Multiple randomized controlled trials have shown that fish oil and its omega-3 polyunsaturated fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) can reduce homocysteine levels, and their effect is augmented by the addition of vitamins B12, B6, and folic acid.126
Omega-3 fatty acids appear to work synergistically with B vitamins to promote healthy homocysteine metabolism and reduce risk of conditions associated with high homocysteine levels, including cardiovascular and neurological diseases.5 Multiple randomized controlled trials have shown that fish oil and its omega-3 polyunsaturated fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) can reduce homocysteine levels, and their effect is augmented by the addition of vitamins B12, B6, and folic acid.126
The beneficial effects of omega-3 fatty acids on cardiovascular and neurological health may depend on adequate homocysteine metabolism. For example, an analysis from one clinical trial in Alzheimer disease patients found treatment with DHA and EPA improved cognitive function only in those with homocysteine levels below 11.7 µmol/L.127 In addition, high levels of omega-3 fatty acids may protect against homocysteine toxicity and enhance the benefits of B vitamins. In one study, high homocysteine levels were linked to increased brain beta-amyloid (a marker of Alzheimer disease risk) in elderly subjects with low omega-3 status, but not those with high omega-3 status.128 Other clinical trials have found B vitamins’ ability to slow brain tissue atrophy and improve cognitive function in individuals with mild cognitive impairment depends on adequate blood levels of omega-3 fatty acids, especially DHA.129,130
N-acetylcysteine
 N-acetylcysteine (NAC) is a source of cysteine that can be used in the body to manufacture the important antioxidant compound, glutathione. By increasing glutathione production and lowering oxidative stress, it is thought NAC might help mitigate some toxic effects of excess homocysteine. In addition, NAC appears to lower homocysteine levels.131,132
N-acetylcysteine (NAC) is a source of cysteine that can be used in the body to manufacture the important antioxidant compound, glutathione. By increasing glutathione production and lowering oxidative stress, it is thought NAC might help mitigate some toxic effects of excess homocysteine. In addition, NAC appears to lower homocysteine levels.131,132
In an eight-week, randomized, controlled trial involving 60 participants with high homocysteine levels and coronary artery disease, 600 mg per day of NAC was as effective as 5 mg per day of folic acid for reducing homocysteine levels compared with placebo.133 Placebo-controlled trials in middle-aged men have found supplementing with 1,800 mg NAC daily for four weeks decreased homocysteine levels by an average of almost 12%. NAC also lowered blood pressure, particularly in those with high cholesterol and triglyceride levels.134 In another trial, 30 patients with high homocysteine levels and Alzheimer disease or a related disorder were treated with a supplement providing undisclosed doses of folate (as 5-MTHF), vitamin B12 (as methylcobalamin), and NAC for periods of time ranging from 2.5 to 34.6 months. Compared to similar patients who received no supplements, brain tissue atrophy in those receiving the B vitamin/NAC combination was substantially reduced.135
Taurine
 Taurine is a non-essential amino acid that, like methionine, cysteine, and homocysteine, is a source of sulfur. Taurine can be made from cysteine in the body and has beneficial effects on vascular, neurological, metabolic, and musculoskeletal health.136,137 Preclinical evidence suggests taurine supplementation may reduce high homocysteine levels and protect heart and blood vessel cells from homocysteine-induced damage.138-140 In a preliminary trial, 22 middle-aged women were given 3 grams per day of taurine for four weeks. This resulted in a drop in average homocysteine level from 8.5 to 7.6 µmol/L.141 Even in subjects with blood homocysteine levels >125 µmol/L due to a genetic disorder called homocystinuria, taurine supplementation was found to improve vascular function.142
Taurine is a non-essential amino acid that, like methionine, cysteine, and homocysteine, is a source of sulfur. Taurine can be made from cysteine in the body and has beneficial effects on vascular, neurological, metabolic, and musculoskeletal health.136,137 Preclinical evidence suggests taurine supplementation may reduce high homocysteine levels and protect heart and blood vessel cells from homocysteine-induced damage.138-140 In a preliminary trial, 22 middle-aged women were given 3 grams per day of taurine for four weeks. This resulted in a drop in average homocysteine level from 8.5 to 7.6 µmol/L.141 Even in subjects with blood homocysteine levels >125 µmol/L due to a genetic disorder called homocystinuria, taurine supplementation was found to improve vascular function.142
S-adenosylmethionine
 S-adenosylmethionine (SAMe) is a crucial methyl donor in many cell processes, including epigenetic gene modification and neurotransmitter synthesis. Since high homocysteine levels are often the result of poor conversion of homocysteine to methionine, which is a precursor of SAMe, SAMe is usually depleted as homocysteine accumulates.8 This may be a contributing factor in the relationship between high homocysteine levels and psycho-emotional conditions such as depression, as well as the higher risk of depression seen in carriers of the MTHFR gene variant associated with impaired folate metabolism.143,144
S-adenosylmethionine (SAMe) is a crucial methyl donor in many cell processes, including epigenetic gene modification and neurotransmitter synthesis. Since high homocysteine levels are often the result of poor conversion of homocysteine to methionine, which is a precursor of SAMe, SAMe is usually depleted as homocysteine accumulates.8 This may be a contributing factor in the relationship between high homocysteine levels and psycho-emotional conditions such as depression, as well as the higher risk of depression seen in carriers of the MTHFR gene variant associated with impaired folate metabolism.143,144
Clinical evidence suggests SAMe may be helpful in treating depression, including in people with elevated homocysteine levels.144,145 One case report described the benefit of SAMe in a patient with anxiety who was found to have a MTHFR gene mutation: treatment with methylated B12 and folate was not effective for relieving symptoms until SAMe, 400 mg twice daily, was added.146 Although concerns have been raised about the possibility that SAMe supplementation might increase homocysteine production, a trial in subjects with major depressive disorder found that 800–1,600 mg per day SAMe for six weeks did not raise homocysteine levels.147
Magnesium
 Magnesium may help counter the negative impacts of high homocysteine levels. Magnesium is well known for protecting against cardiovascular conditions such as high blood pressure, atherosclerosis, arrhythmias, coronary artery disease, and heart failure, and numerous studies have demonstrated the association between magnesium intake and reduced risk of heart attack and stroke.148,149 Research further shows magnesium may be helpful in protecting cognitive function and neurological health in general.150
Magnesium may help counter the negative impacts of high homocysteine levels. Magnesium is well known for protecting against cardiovascular conditions such as high blood pressure, atherosclerosis, arrhythmias, coronary artery disease, and heart failure, and numerous studies have demonstrated the association between magnesium intake and reduced risk of heart attack and stroke.148,149 Research further shows magnesium may be helpful in protecting cognitive function and neurological health in general.150
Findings from a laboratory study suggest low magnesium status may exacerbate the intracellular magnesium loss triggered by homocysteine.151 Another study in blood vessel cells cultured in a laboratory found homocysteine increased production of compounds that trigger structural changes associated with plaque formation; however, adding magnesium to the cells’ environment mitigated this atherogenic effect of homocysteine.152 Magnesium has also been shown to reverse the adverse effect of homocysteine on cardiac rhythm in laboratory mice.153
Material used with permission of Life Extension. All rights reserved.
- Esse R, Barroso M, Tavares de Almeida I, Castro R. The Contribution of Homocysteine Metabolism Disruption to Endothelial Dysfunction: State-of-the-Art. International journal of molecular sciences. 2019;20(4).
- Tinelli C, Di Pino A, Ficulle E, Marcelli S, Feligioni M.
- Hyperhomocysteinemia as a Risk Factor and Potential Nutraceutical Target for Certain Pathologies. Frontiers in nutrition. 2019;6:49.
- Zaric BL, Obradovic M, Bajic V, Haidara MA, Jovanovic M, Isenovic ER. Homocysteine and Hyperhomocysteinaemia. Curr Med Chem. 2019;26(16):2948-2961.
- Troesch B, Weber P, Mohajeri MH. Potential Links between Impaired One-Carbon Metabolism Due to Polymorphisms, Inadequate B-Vitamin Status, and the Development of Alzheimer's Disease. Nutrients. 2016;8(12).
- Rizzo G, Lagana AS. The Link between Homocysteine and Omega-3 Polyunsaturated Fatty Acid: Critical Appraisal and Future Directions. Biomolecules. 2020;10(2).
- Komorniak N, Szczuko M, Kowalewski B, Stachowska E. Nutritional Deficiencies, Bariatric Surgery, and Serum Homocysteine Level: Review of Current Literature. Obesity surgery. 2019;29(11):3735-3742.
- Froese DS, Fowler B, Baumgartner MR. Vitamin B12 , folate, and the methionine remethylation cycle-biochemistry, pathways, and regulation. Journal of inherited metabolic disease. 2019;42(4):673-685.
- Fu Y, Wang X, Kong W. Hyperhomocysteinaemia and vascular injury: advances in mechanisms and drug targets. Br J Pharmacol. 2018;175(8):1173-1189.
- Yang Q, He GW. Imbalance of Homocysteine and H2S: Significance, Mechanisms, and Therapeutic Promise in Vascular Injury. Oxid Med Cell Longev. 2019;2019:7629673.
- Ganguly P, Alam SF. Role of homocysteine in the development of cardiovascular disease. Nutr J. 2015;14:6.
- Ledda C, Cannizzaro E, Lovreglio P, et al. Exposure to Toxic Heavy Metals Can Influence Homocysteine Metabolism? Antioxidants (Basel, Switzerland). 2019;9(1).
- Hankey GJ. B vitamins for stroke prevention. Stroke Vasc Neurol. 2018;3(2):51-58.
- Urgert R, van Vliet T, Zock PL, Katan MB. Heavy coffee consumption and plasma homocysteine: a randomized controlled trial in healthy volunteers. Am J Clin Nutr. 2000;72(5):1107-1110.
- Miller JW. Proton Pump Inhibitors, H2-Receptor Antagonists, Metformin, and Vitamin B-12 Deficiency: Clinical Implications. Adv Nutr. 2018;9(4):511s-518s.
- Dierkes J, Luley C, Westphal S. Effect of lipid-lowering and anti-hypertensive drugs on plasma homocysteine levels. Vasc Health Risk Manag. 2007;3(1):99-108.
- Djuric D, Jakovljevic V, Zivkovic V, Srejovic I. Homocysteine and homocysteine-related compounds: an overview of the roles in the pathology of the cardiovascular and nervous systems. Canadian journal of physiology and pharmacology. 2018;96(10):991-1003.
- Jakubowski H. Homocysteine Modification in Protein Structure/Function and Human Disease. Physiol Rev. 2019;99(1):555-604.
- Zhu M, Mao M, Lou X. Elevated homocysteine level and prognosis in patients with acute coronary syndrome: a meta-analysis. Biomarkers. 2019;24(4):309-316.
- Peng HY, Man CF, Xu J, Fan Y. Elevated homocysteine levels and risk of cardiovascular and all-cause mortality: a meta-analysis of prospective studies. Journal of Zhejiang University Science B. 2015;16(1):78-86.
- Ma Y, Peng D, Liu C, Huang C, Luo J. Serum high concentrations of homocysteine and low levels of folic acid and vitamin B12 are significantly correlated with the categories of coronary artery diseases. BMC cardiovascular disorders. 2017;17(1):37.
- Alam SF, Kumar S, Ganguly P. Measurement of homocysteine: a historical perspective. Journal of clinical biochemistry and nutrition. 2019;65(3):171-177.
- Li S, Pan G, Chen H, Niu X. Determination of Serum Homocysteine and Hypersensitive C-reactive Protein and Their Correlation with Premature Coronary Heart Disease. Heart Surg Forum. 2019;22(3):E215-e217.
- Wei M, Wang L, Liu YS, et al. Homocysteine as a potential predictive factor for high major adverse cardiovascular events risk in female patients with premature acute coronary syndrome. Medicine. 2019;98(47):e18019.
- Moretti R, Peinkhofer C. B Vitamins and Fatty Acids: What Do They Share with Small Vessel Disease-Related Dementia? International journal of molecular sciences. 2019;20(22).
- Spence JD. Cardioembolic stroke: everything has changed. Stroke Vasc Neurol. 2018;3(2):76-83.
- Moretti R, Caruso P. The Controversial Role of Homocysteine in Neurology: From Labs to Clinical Practice. International journal of molecular sciences. 2019;20(1).
- Spence JD. Homocysteine lowering for stroke prevention: Unravelling the complexity of the evidence. Int J Stroke. 2016;11(7):744-747.
- Smith AD, Refsum H, Bottiglieri T, et al. Homocysteine and Dementia: An International Consensus Statement. J Alzheimers Dis. 2018;62(2):561-570.
- Zhou F, Chen S. Hyperhomocysteinemia and risk of incident cognitive outcomes: An updated dose-response meta-analysis of prospective cohort studies. Ageing Res Rev. 2019;51:55-66.
- Licking N, Murchison C, Cholerton B, et al. Homocysteine and cognitive function in Parkinson's disease. Parkinsonism Relat Disord. 2017;44:1-5.
- Hasan T, Arora R, Bansal AK, Bhattacharya R, Sharma GS, Singh LR. Disturbed homocysteine metabolism is associated with cancer. Experimental & molecular medicine. 2019;51(2):21.
- Lei X, Zeng G, Zhang Y, et al. Association between homocysteine level and the risk of diabetic retinopathy: a systematic review and meta-analysis. Diabetol Metab Syndr. 2018;10:61.
- Mao S, Xiang W, Huang S, Zhang A. Association between homocysteine status and the risk of nephropathy in type 2 diabetes mellitus. Clin Chim Acta. 2014;431:206-210.
- Sansone A, Cignarelli A, Sansone M, et al. Serum Homocysteine Levels in Men with and without Erectile Dysfunction: A Systematic Review and Meta-Analysis. International journal of endocrinology. 2018;2018:7424792.
- Gaiday AN, Tussupkaliyev AB, Bermagambetova SK, et al. Effect of homocysteine on pregnancy: A systematic review. Chem Biol Interact. 2018;293:70-76.
- Iacobazzi V, Infantino V, Castegna A, Andria G. Hyperhomocysteinemia: related genetic diseases and congenital defects, abnormal DNA methylation and newborn screening issues. Molecular genetics and metabolism. 2014;113(1-2):27-33.
- Saito M, Marumo K. The Effects of Homocysteine on the Skeleton. Current osteoporosis reports. 2018;16(5):554-560.
- Partearroyo T, Vallecillo N, Pajares MA, Varela-Moreiras G, Varela-Nieto I. Cochlear Homocysteine Metabolism at the Crossroad of Nutrition and Sensorineural Hearing Loss. Frontiers in molecular neuroscience. 2017;10:107.
- Pinna A, Zaccheddu F, Boscia F, Carru C, Solinas G. Homocysteine and risk of age-related macular degeneration: a systematic review and meta-analysis. Acta Ophthalmol. 2018;96(3):e269-e276.
- Pizzorno J. Homocysteine: Friend or Foe? Integrative medicine (Encinitas, Calif). 2014;13(4):8-14.
- Refsum H, Nurk E, Smith AD, et al. The Hordaland Homocysteine Study: a community-based study of homocysteine, its determinants, and associations with disease. J Nutr. 2006;136(6 Suppl):1731s-1740s.
- Nurk E, Tell GS, Vollset SE, Nygard O, Refsum H, Ueland PM. Plasma total homocysteine and hospitalizations for cardiovascular disease: the Hordaland Homocysteine Study. Arch Intern Med. 2002;162(12):1374-1381.
- Nygard O, Nordrehaug JE, Refsum H, Ueland PM, Farstad M, Vollset SE. Plasma homocysteine levels and mortality in patients with coronary artery disease. The New England journal of medicine. 1997;337(4):230-236.
- Vollset SE, Refsum H, Tverdal A, et al. Plasma total homocysteine and cardiovascular and noncardiovascular mortality: the Hordaland Homocysteine Study. Am J Clin Nutr. 2001;74(1):130-136.
- Iso H, Moriyama Y, Sato S, et al. Serum total homocysteine concentrations and risk of stroke and its subtypes in Japanese. Circulation. 2004;109(22):2766-2772.
- Seshadri S, Beiser A, Selhub J, et al. Plasma homocysteine as a risk factor for dementia and Alzheimer's disease. The New England journal of medicine. 2002;346(7):476-483.
- Clarke R, Birks J, Nexo E, et al. Low vitamin B-12 status and risk of cognitive decline in older adults. Am J Clin Nutr. 2007;86(5):1384-1391.
- Smith AD, Smith SM, de Jager CA, et al. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One. 2010;5(9):e12244.
- Ward M, McNulty H, McPartlin J, Strain JJ, Weir DG, Scott JM. Plasma homocysteine, a risk factor for cardiovascular disease, is lowered by physiological doses of folic acid. Qjm. 1997;90(8):519-524.
- Rai V. Methylenetetrahydrofolate Reductase (MTHFR) C677T Polymorphism and Alzheimer Disease Risk: a Meta-Analysis. Molecular neurobiology. 2017;54(2):1173-1186.
- Reilly R, McNulty H, Pentieva K, Strain JJ, Ward M. MTHFR 677TT genotype and disease risk: is there a modulating role for B-vitamins? The Proceedings of the Nutrition Society. 2014;73(1):47-56.
- Du B, Tian H, Tian D, et al. Genetic polymorphisms of key enzymes in folate metabolism affect the efficacy of folate therapy in patients with hyperhomocysteinaemia. The British journal of nutrition. 2018;119(8):887-895.
- Garcia-Minguillan CJ, Fernandez-Ballart JD, Ceruelo S, et al. Riboflavin status modifies the effects of methylenetetrahydrofolate reductase (MTHFR) and methionine synthase reductase (MTRR) polymorphisms on homocysteine. Genes Nutr. 2014;9(6):435.
- Ding R, Lin S, Chen D. The association of cystathionine β synthase (CBS) T833C polymorphism and the risk of stroke: a meta-analysis. J Neurol Sci. 2012;312(1-2):26-30.
- Bublil EM, Majtan T. Classical homocystinuria: From cystathionine beta-synthase deficiency to novel enzyme therapies. Biochimie. 2019.
- Delchier N, Ringling C, Maingonnat JF, Rychlik M, Renard CM. Mechanisms of folate losses during processing: diffusion vs. heat degradation. Food Chem. 2014;157:439-447.
- ter Borg S, Verlaan S, Hemsworth J, et al. Micronutrient intakes and potential inadequacies of community-dwelling older adults: a systematic review. The British journal of nutrition. 2015;113(8):1195-1206.
- Sobczynska-Malefora A, Harrington DJ. Laboratory assessment of folate (vitamin B9) status. Journal of clinical pathology. 2018;71(11):949-956.
- Baroni L, Bonetto C, Rizzo G, Bertola C, Caberlotto L, Bazzerla G. Association Between Cognitive Impairment and Vitamin B12, Folate, and Homocysteine Status in Elderly Adults: A Retrospective Study. J Alzheimers Dis. 2019;70(2):443-453.
- Robinson N, Grabowski P, Rehman I. Alzheimer's disease pathogenesis: Is there a role for folate? Mech Ageing Dev. 2018;174:86-94.
- Li Y, Huang T, Zheng Y, Muka T, Troup J, Hu FB. Folic Acid Supplementation and the Risk of Cardiovascular Diseases: A Meta-Analysis of Randomized Controlled Trials. J Am Heart Assoc. 2016;5(8).
- Enderami A, Zarghami M, Darvishi-Khezri H. The effects and potential mechanisms of folic acid on cognitive function: a comprehensive review. Neurol Sci. 2018;39(10):1667-1675.
- Tian T, Yang KQ, Cui JG, Zhou LL, Zhou XL. Folic Acid Supplementation for Stroke Prevention in Patients With Cardiovascular Disease. The American journal of the medical sciences. 2017;354(4):379-387.
- Wang WW, Wang XS, Zhang ZR, He JC, Xie CL. A Meta-Analysis of Folic Acid in Combination with Anti-Hypertension Drugs in Patients with Hypertension and Hyperhomocysteinemia. Frontiers in pharmacology. 2017;8:585.
- Akbari M, Tabrizi R, Lankarani KB, et al. The Effects of Folate Supplementation on Diabetes Biomarkers Among Patients with Metabolic Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Hormone and metabolic research = Hormon- und Stoffwechselforschung = Hormones et metabolisme. 2018;50(2):93-105.
- Tabrizi R, Lankarani KB, Akbari M, et al. The effects of folate supplementation on lipid profiles among patients with metabolic diseases: A systematic review and meta-analysis of randomized controlled trials. Diabetes Metab Syndr. 2018;12(3):423-430.
- GARD. MTHFR gene variant. NIH. rarediseases.info.nih.gov Web site. https://rarediseases.info.nih.gov/diseases/10953/mthfr-gene-mutation. Published 2019. Accessed 05/12/2020.
- Scaglione F, Panzavolta G. Folate, folic acid and 5-methyltetrahydrofolate are not the same thing. Xenobiotica; the fate of foreign compounds in biological systems. 2014;44(5):480-488.
- Servy E, Menezo Y. The Methylene Tetrahydrofolate Reductase (MTHFR) isoform challenge. High doses of folic acid are not a suitable option compared to 5 Methyltetrahydrofolate treatment. Clinical Obstetrics, Gynecology and Reproductive Medicine. 2017;3:1-5.
- Prinz-Langenohl R, Brämswig S, Tobolski O, et al. [6S]-5-methyltetrahydrofolate increases plasma folate more effectively than folic acid in women with the homozygous or wild-type 677C-->T polymorphism of methylenetetrahydrofolate reductase. Br J Pharmacol. 2009;158(8):2014-2021.
- Willems FF, Boers GH, Blom HJ, Aengevaeren WR, Verheugt FW. Pharmacokinetic study on the utilisation of 5-methyltetrahydrofolate and folic acid in patients with coronary artery disease. Br J Pharmacol. 2004;141(5):825-830.
- Henderson AM, Aleliunas RE, Loh SP, et al. l-5-Methyltetrahydrofolate Supplementation Increases Blood Folate Concentrations to a Greater Extent than Folic Acid Supplementation in Malaysian Women. J Nutr. 2018;148(6):885-890.
- Venn BJ, Green TJ, Moser R, Mann JI. Comparison of the effect of low-dose supplementation with L-5-methyltetrahydrofolate or folic acid on plasma homocysteine: a randomized placebo-controlled study. Am J Clin Nutr. 2003;77(3):658-662.
- Lamers Y, Prinz-Langenohl R, Bramswig S, Pietrzik K. Red blood cell folate concentrations increase more after supplementation with [6S]-5-methyltetrahydrofolate than with folic acid in women of childbearing age. Am J Clin Nutr. 2006;84(1):156-161.
- Cornet D, Clement A, Clement P, Menezo Y. High doses of folic acid induce a pseudo-methylenetetrahydrofolate syndrome. SAGE Open Med Case Rep. 2019;7:2050313x19850435.
- Tafuri L, Servy E, Menezo Y. The hazards of excessive folic acid intake in MTHFR gene mutation carriers: An obstetric and gynecological perspective. Clinical Obstetrics, Gynecology and Reproductive Medicine. 2018;4:1-2.
- Calderon-Ospina CA, Nava-Mesa MO. B Vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS neuroscience & therapeutics. 2020;26(1):5-13.
- Wolffenbuttel BHR, Wouters H, Heiner-Fokkema MR, van der Klauw MM. The Many Faces of Cobalamin (Vitamin B12) Deficiency. Mayo Clin Proc Innov Qual Outcomes. 2019;3(2):200-214.
- Wang H, Li L, Qin LL, Song Y, Vidal-Alaball J, Liu TH. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. The Cochrane database of systematic reviews. 2018;3:Cd004655.
- Roman GC, Mancera-Paez O, Bernal C. Epigenetic Factors in Late-Onset Alzheimer's Disease: MTHFR and CTH Gene Polymorphisms, Metabolic Transsulfuration and Methylation Pathways, and B Vitamins. International journal of molecular sciences. 2019;20(2).
- Obeid R, Heil SG, Verhoeven MMA, van den Heuvel E, de Groot L, Eussen S. Vitamin B12 Intake From Animal Foods, Biomarkers, and Health Aspects. Frontiers in nutrition. 2019;6:93.
- NIH. National Institutes of Health. Vitamin B12 Level. US National Library of Medicine: Medline Plus. Available at https://medlineplus.gov/ency/article/003705.htm. Last update 1/19/2018. Accessed 01/25/2020. 2018.
- Field MS, Stover PJ. Safety of folic acid. Ann N Y Acad Sci. 2018;1414(1):59-71.
- Eussen SJ, de Groot LC, Clarke R, et al. Oral cyanocobalamin supplementation in older people with vitamin B12 deficiency: a dose-finding trial. Arch Intern Med. 2005;165(10):1167-1172.
- Kennedy DO. B Vitamins and the Brain: Mechanisms, Dose and Efficacy--A Review. Nutrients. 2016;8(2):68.
- Watson J, Lee M, Garcia-Casal MN. Consequences of Inadequate Intakes of Vitamin A, Vitamin B12, Vitamin D, Calcium, Iron, and Folate in Older Persons. Curr Geriatr Rep. 2018;7(2):103-113.
- Pavlov CS, Damulin IV, Shulpekova YO, Andreev EA. Neurological disorders in vitamin B12 deficiency. Terapevticheskii arkhiv. 2019;91(4):122-129.
- Parra M, Stahl S, Hellmann H. Vitamin B(6) and Its Role in Cell Metabolism and Physiology. Cells. 2018;7(7).
- Jayedi A, Zargar MS. Intake of vitamin B6, folate, and vitamin B12 and risk of coronary heart disease: a systematic review and dose-response meta-analysis of prospective cohort studies. Crit Rev Food Sci Nutr. 2019;59(16):2697-2707.
- Wilson MP, Plecko B, Mills PB, Clayton PT. Disorders affecting vitamin B6 metabolism. Journal of inherited metabolic disease. 2019;42(4):629-646.
- Vrolijk MF, Opperhuizen A, Jansen E, Hageman GJ, Bast A, Haenen G. The vitamin B6 paradox: Supplementation with high concentrations of pyridoxine leads to decreased vitamin B6 function. Toxicol In Vitro. 2017;44:206-212.
- Porter K, Hoey L, Hughes CF, Ward M, McNulty H. Causes, Consequences and Public Health Implications of Low B-Vitamin Status in Ageing. Nutrients. 2016;8(11).
- Marashly ET, Bohlega SA. Riboflavin Has Neuroprotective Potential: Focus on Parkinson's Disease and Migraine. Frontiers in neurology. 2017;8:333.
- Douaud G, Refsum H, de Jager CA, et al. Preventing Alzheimer's disease-related gray matter atrophy by B-vitamin treatment. Proc Natl Acad Sci U S A. 2013;110(23):9523-9528.
- Mazza A, Cicero AF, Ramazzina E, et al. Nutraceutical approaches to homocysteine lowering in hypertensive subjects at low cardiovascular risk: a multicenter, randomized clinical trial. Journal of biological regulators and homeostatic agents. 2016;30(3):921-927.
- Han L, Liu Y, Wang C, et al. Determinants of hyperhomocysteinemia in healthy and hypertensive subjects: A population-based study and systematic review. Clin Nutr. 2017;36(5):1215-1230.
- Kose S, Sozlu S, Bolukbasi H, Unsal N, Gezmen-Karadag M. Obesity is associated with folate metabolism. International journal for vitamin and nutrition research Internationale Zeitschrift fur Vitamin- und Ernahrungsforschung Journal international de vitaminologie et de nutrition. 2019:1-12.
- Zappacosta B, Mastroiacovo P, Persichilli S, et al. Homocysteine lowering by folate-rich diet or pharmacological supplementations in subjects with moderate hyperhomocysteinemia. Nutrients. 2013;5(5):1531-1543.
- Gibson A, Woodside JV, Young IS, et al. Alcohol increases homocysteine and reduces B vitamin concentration in healthy male volunteers--a randomized, crossover intervention study. Qjm. 2008;101(11):881-887.
- Kumar A, Palfrey HA, Pathak R, Kadowitz PJ, Gettys TW, Murthy SN. The metabolism and significance of homocysteine in nutrition and health. Nutrition & Metabolism. 2017;14(1):78.
- Pawlak R. Is vitamin B12 deficiency a risk factor for cardiovascular disease in vegetarians? Am J Prev Med. 2015;48(6):e11-26.
- Obersby D, Chappell DC, Dunnett A, Tsiami AA. Plasma total homocysteine status of vegetarians compared with omnivores: a systematic review and meta-analysis. The British journal of nutrition. 2013;109(5):785-794.
- Foscolou A, Rallidis LS, Tsirebolos G, et al. The association between homocysteine levels, Mediterranean diet and cardiovascular disease: a case-control study. International journal of food sciences and nutrition. 2019;70(5):603-611.
- Visekruna I, Rumbak I, Samarin IR, Keser I, Ranilovic J. Homocysteine Levels Show Significant Differences among Mediterranean Dietary Quality Index Variables Compared to Folate and Vitamin B(12) Status in Women. International journal for vitamin and nutrition research Internationale Zeitschrift fur Vitamin- und Ernahrungsforschung Journal international de vitaminologie et de nutrition. 2015;85(3-4):202-210.
- Teixeira JA, Steluti J, Gorgulho BM, et al. Prudent dietary pattern influences homocysteine level more than folate, vitamin B12, and docosahexaenoic acid: a structural equation model approach. European journal of nutrition. 2019.
- Maroto-Sanchez B, Lopez-Torres O, Palacios G, Gonzalez-Gross M. What do we know about homocysteine and exercise? A review from the literature. Clinical chemistry and laboratory medicine : CCLM / FESCC. 2016;54(10):1561-1577.
- Maroto-Sanchez B, Lopez-Torres O, Valtuena J, et al. Rehydration during exercise prevents the increase of homocysteine concentrations. Amino Acids. 2019;51(2):193-204.
- Deminice R, Ribeiro DF, Frajacomo FT. The Effects of Acute Exercise and Exercise Training on Plasma Homocysteine: A Meta-Analysis. PLoS One. 2016;11(3):e0151653.
- Buckner SL, Loenneke JP, Loprinzi PD. Single and combined associations of accelerometer-assessed physical activity and muscle-strengthening activities on plasma homocysteine in a national sample. Clin Physiol Funct Imaging. 2017;37(6):669-674.
- Alomari MA, Khabour OF, Gharaibeh MY, Qhatan RA. Effect of physical activity on levels of homocysteine, folate, and vitamin B12 in the elderly. The Physician and sportsmedicine. 2016;44(1):68-73.
- Kuebler U, Linnebank M, Semmler A, et al. Plasma homocysteine levels increase following stress in older but not younger men. Psychoneuroendocrinology. 2013;38(8):1381-1387.
- Chien LW, Chang HC, Liu CF. Effect of yoga on serum homocysteine and nitric oxide levels in adolescent women with and without dysmenorrhea. Journal of alternative and complementary medicine (New York, NY). 2013;19(1):20-23.
- Ueland PM. Choline and betaine in health and disease. Journal of inherited metabolic disease. 2011;34(1):3-15.
- Craig SA. Betaine in human nutrition. The American Journal of Clinical Nutrition. 2004;80(3):539-549.
- Zeisel S. Choline, Other Methyl-Donors and Epigenetics. Nutrients. 2017;9(5).
- Obeid R. The metabolic burden of methyl donor deficiency with focus on the betaine homocysteine methyltransferase pathway. Nutrients. 2013;5(9):3481-3495.
- Lee JE, Jacques PF, Dougherty L, et al. Are dietary choline and betaine intakes determinants of total homocysteine concentration? Am J Clin Nutr. 2010;91(5):1303-1310.
- Wallace TC, Fulgoni VL, 3rd. Assessment of Total Choline Intakes in the United States. J Am Coll Nutr. 2016;35(2):108-112.
- Atkinson W, Slow S, Elmslie J, Lever M, Chambers ST, George PM. Dietary and supplementary betaine: effects on betaine and homocysteine concentrations in males. Nutr Metab Cardiovasc Dis. 2009;19(11):767-773.
- Olthof MR, Verhoef P. Effects of betaine intake on plasma homocysteine concentrations and consequences for health. Curr Drug Metab. 2005;6(1):15-22.
- Steenge GR, Verhoef P, Katan MB. Betaine supplementation lowers plasma homocysteine in healthy men and women. J Nutr. 2003;133(5):1291-1295.
- Jakubowski H, Glowacki R. Chemical biology of homocysteine thiolactone and related metabolites. Advances in clinical chemistry. 2011;55:81-103.
- Cholewa JM, Wyszczelska-Rokiel M, Glowacki R, et al. Effects of betaine on body composition, performance, and homocysteine thiolactone. Journal of the International Society of Sports Nutrition. 2013;10(1):39.
- Guasch-Ferre M, Hu FB, Ruiz-Canela M, et al. Plasma Metabolites From Choline Pathway and Risk of Cardiovascular Disease in the PREDIMED (Prevention With Mediterranean Diet) Study. J Am Heart Assoc. 2017;6(11).
- Meyer KA, Shea JW. Dietary Choline and Betaine and Risk of CVD: A Systematic Review and Meta-Analysis of Prospective Studies. Nutrients. 2017;9(7).
- Dawson SL, Bowe SJ, Crowe TC. A combination of omega-3 fatty acids, folic acid and B-group vitamins is superior at lowering homocysteine than omega-3 alone: A meta-analysis. Nutr Res. 2016;36(6):499-508.
- Jerneren F, Cederholm T, Refsum H, et al. Homocysteine Status Modifies the Treatment Effect of Omega-3 Fatty Acids on Cognition in a Randomized Clinical Trial in Mild to Moderate Alzheimer's Disease: The OmegAD Study. J Alzheimers Dis. 2019;69(1):189-197.
- Hooper C, De Souto Barreto P, Coley N, et al. Cross-Sectional Associations of Total Plasma Homocysteine with Cortical beta-Amyloid Independently and as a Function of Omega 3 Polyunsaturated Fatty Acid Status in Older Adults at Risk of Dementia. The journal of nutrition, health & aging. 2017;21(10):1075-1080.
- Jerneren F, Elshorbagy AK, Oulhaj A, Smith SM, Refsum H, Smith AD. Brain atrophy in cognitively impaired elderly: the importance of long-chain omega-3 fatty acids and B vitamin status in a randomized controlled trial. Am J Clin Nutr. 2015;102(1):215-221.
- Oulhaj A, Jerneren F, Refsum H, Smith AD, de Jager CA. Omega-3 Fatty Acid Status Enhances the Prevention of Cognitive Decline by B Vitamins in Mild Cognitive Impairment. J Alzheimers Dis. 2016;50(2):547-557.
- Aydin AF, Kondakci G, Hatipoglu S, Dogru-Abbasoglu S, Uysal M. N-Acetylcysteine supplementation decreased brain lipid and protein oxidations produced by experimental homocysteine thiolactone exposure: Relevance to neurodegeneration. Pathophysiology : the official journal of the International Society for Pathophysiology. 2018;25(2):125-129.
- Kondakci G, Aydin AF, Dogru-Abbasoglu S, Uysal M. The effect of N-acetylcysteine supplementation on serum homocysteine levels and hepatic and renal oxidative stress in homocysteine thiolactone-treated rats. Arch Physiol Biochem. 2017;123(2):128-133.
- Yilmaz H, Sahin S, Sayar N, et al. Effects of folic acid and N-acetylcysteine on plasma homocysteine levels and endothelial function in patients with coronary artery disease. Acta cardiologica. 2007;62(6):579-585.
- Hildebrandt W, Sauer R, Bonaterra G, Dugi KA, Edler L, Kinscherf R. Oral N-acetylcysteine reduces plasma homocysteine concentrations regardless of lipid or smoking status. Am J Clin Nutr. 2015;102(5):1014-1024.
- Shankle WR, Hara J, Barrentine LW, Curole MV. CerefolinNAC Therapy of Hyperhomocysteinemia Delays Cortical and White Matter Atrophy in Alzheimer's Disease and Cerebrovascular Disease. J Alzheimers Dis. 2016;54(3):1073-1084.
- Schaffer S, Kim HW. Effects and Mechanisms of Taurine as a Therapeutic Agent. Biomolecules & therapeutics. 2018;26(3):225-241.
- Jakaria M, Azam S, Haque ME, et al. Taurine and its analogs in neurological disorders: Focus on therapeutic potential and molecular mechanisms. Redox biology. 2019;24:101223.
- Zulli A, Lau E, Wijaya BP, et al. High dietary taurine reduces apoptosis and atherosclerosis in the left main coronary artery: association with reduced CCAAT/enhancer binding protein homologous protein and total plasma homocysteine but not lipidemia. Hypertension. 2009;53(6):1017-1022.
- Nonaka H, Tsujino T, Watari Y, Emoto N, Yokoyama M. Taurine prevents the decrease in expression and secretion of extracellular superoxide dismutase induced by homocysteine: amelioration of homocysteine-induced endoplasmic reticulum stress by taurine. Circulation. 2001;104(10):1165-1170.
- Zhang Z, Zhao L, Zhou Y, et al. Taurine ameliorated homocysteine-induced H9C2 cardiomyocyte apoptosis by modulating endoplasmic reticulum stress. Apoptosis. 2017;22(5):647-661.
- Ahn CS. Effect of taurine supplementation on plasma homocysteine levels of the middle-aged Korean women. Adv Exp Med Biol. 2009;643:415-422.
- an Hove JLK, Freehauf CL, Ficicioglu C, et al. Biomarkers of oxidative stress, inflammation, and vascular dysfunction in inherited cystathionine beta-synthase deficient homocystinuria and the impact of taurine treatment in a phase 1/2 human clinical trial. Journal of inherited metabolic disease. 2019;42(3):424-437.
- Bhatia P, Singh N. Homocysteine excess: delineating the possible mechanism of neurotoxicity and depression. Fundamental & clinical pharmacology. 2015;29(6):522-528.
- Papakostas GI, Cassiello CF, Iovieno N. Folates and S-adenosylmethionine for major depressive disorder. Can J Psychiatry. 2012;57(7):406-413.
- Karas Kuzelicki N. S-Adenosyl Methionine in the Therapy of Depression and Other Psychiatric Disorders. Drug Dev Res. 2016;77(7):346-356.
- Anderson S, Panka J, Rakobitsch R, Tyre K, Pulliam K. Anxiety and Methylenetetrahydrofolate Reductase Mutation Treated With S-Adenosyl Methionine and Methylated B Vitamins. Integrative medicine (Encinitas, Calif). 2016;15(2):48-52.
- Mischoulon D, Alpert JE, Arning E, Bottiglieri T, Fava M, Papakostas GI. Bioavailability of S-adenosyl methionine and impact on response in a randomized, double-blind, placebo-controlled trial in major depressive disorder. The Journal of clinical psychiatry. 2012;73(6):843-848.
- Zhao L, Hu M, Yang L, et al. Quantitative Association Between Serum/Dietary Magnesium and Cardiovascular Disease/Coronary Heart Disease Risk: A Dose-Response Meta-analysis of Prospective Cohort Studies. Journal of cardiovascular pharmacology. 2019;74(6):516-527.
- Rosique-Esteban N, Guasch-Ferre M, Hernandez-Alonso P, Salas-Salvado J. Dietary Magnesium and Cardiovascular Disease: A Review with Emphasis in Epidemiological Studies. Nutrients. 2018;10(2).
- Kirkland AE, Sarlo GL, Holton KF. The Role of Magnesium in Neurological Disorders. Nutrients. 2018;10(6).
- Li W, Zheng T, Wang J, Altura BT, Altura BM. Extracellular magnesium regulates effects of vitamin B6, B12 and folate on homocysteinemia-induced depletion of intracellular free magnesium ions in canine cerebral vascular smooth muscle cells: possible relationship to [Ca2+]i, atherogenesis and stroke. Neurosci Lett. 1999;274(2):83-86.
- Guo H, Lee JD, Uzui H, et al. Effects of folic acid and magnesium on the production of homocysteine-induced extracellular matrix metalloproteinase-2 in cultured rat vascular smooth muscle cells. Circulation journal : official journal of the Japanese Circulation Society. 2006;70(1):141-146.
- Soni CV, Tyagi SC, Todnem ND, et al. Hyperhomocysteinemia Alters Sinoatrial and Atrioventricular Nodal Function: Role of Magnesium in Attenuating These Effects. Cell Biochem Biophys. 2016;74(1):59-65.
Related product
-
Homocysteine Resist
Price: 25,90 €This formulation combines vitamins B2, B6 and B12, plus folate as L-5-MTHF...
Related posts
-
 Is Conventional Pomegranate Extract Enough?
An abundance of clinical data has established pomegranate as a broad-spectrum, multi-modal defense against the...
Is Conventional Pomegranate Extract Enough?
An abundance of clinical data has established pomegranate as a broad-spectrum, multi-modal defense against the... -
Lipoic Acid Reverses Mitochondrial Decay
It is estimated that 85% of the oxygen contained in every breath you take is consumed by the mitochondria within each...
-
Vitamin C and Dihydroquercetin
Every day, our bodies are under continual assault by damaging agents known as free radicals. Generally, both internal...
-
How Resveratrol Combats Leading Causes of Death
In 1997, the first scientific paper on resveratrol was published showing that this polyphenol could prevent cancer in...
-
Cukrzyca opis choroby Część 2
Cukrzycy typu 1 potrzebują dożywotniej insulinoterapii, choć suplementy wymienione w niniejszym rozdziale mogą pomóc...